
This article is working document and is open to queries and corrections. Email panda@pandata.org
In the previous articles of this mini series about excess deaths we looked at how effective the Covid shots were at arresting Covid [1, 2] and also how bad the “first wave” in New York city was.[3] There are good reasons behind why we chose to address these two topics first. One reason is that an honest look at these issues helps establish a balanced understanding of what might be driving excess deaths since 2020. Another reason is that both topics were central to the official narrative emanating from government sources and the mainstream media. We were told that the whole point of the lockdowns was to delay the spread of SARS-CoV-2 until a vaccine could be developed that would spare us from overwhelmed hospitals like what happened in places like New York and Italy.
As has been shown, and to put it mildly, the Covid shots did not perform nearly as well as promised. Sadly, the burden of the adverse events caused by the experimental shots turned out to be worse than the disease.[4] Furthermore, by a close examination of excess deaths in New York city in early 2020, and in particular by a comparison to what happened on the Diamond Princess, it was concluded that the tragedy in New York was not compatible with the spread of a virus such as SARS-CoV-2, let alone any other generally mild respiratory virus.
All of this presses us to take a step back and address the central theme of the Covid-era narrative, namely the idea that SARS-CoV-2 is a novel virus that is particularly deadly; so deadly that drastic measures were needed to contain it. We begin with a look at the idea that the virus is novel.
How is it possible that a mortality analysis seems to contradict reports about millions of Covid cases and deaths?
1. How novel is SARS-CoV-2?
In the field of virology, the term “novel virus” typically means that the virus was recently discovered. This definition, of course, tells us nothing at all about when the virus first existed. Thus, for instance, the first human-coronavirus was found in 1961.[5] It was labeled B814 and identified as a cause of the common cold. This does not mean that this particular cold-causing coronavirus suddenly appeared in that year. No, and much to the rather, it only means someone finally found it. The ability to isolate, identify and sequence RNA viruses is a relatively new science. The patent on the process used in PCR machines was first granted in 1987.[6] It was in 2003, only 20 years ago, that the first human reference genome was sequenced. Despite all the efforts by many scientists, mankind has not yet sequenced every virus on planet earth. It is quite possible we never will. As a result, we are hardly in a position to assert when a particular virus (or strain of a virus) first appeared. Even if sequencing of a virus could prove beyond reasonable doubt that it was made in a laboratory, unless we had lab records to prove when it was made, it would still be nearly impossible to determine when it first infected someone. At best we might be able to estimate a timeframe by using antibody tests applied to stored specimens. The fact that SARS-CoV-2 is a relatively mild virus with symptoms similar to that caused by the flu only compounds the challenge. All we know for certain about this virus is that labs first began testing for it in early 2020.
The real problem with all of this is that during the Covid era the term “novel virus” was used by many outlets (including universities, journals, the media, and government officials) to mean something quite different from “recently discovered.”[7] For example, the GoodRx website has an article in which the authors say that “SARS-CoV-2, the virus that causes COVID-19, is a “novel coronavirus.” This means it’s different from all viruses like it.” They go on to say that “In medicine, novel refers to a virus or bacteria that wasn’t known to affect humans. This means that the bug is either brand new or was only found in animals or other life forms.” [8] Likewise, Dr. Tam, the chief medical officer of Canada, recently wrote, “In March 2020, Canada was faced with a… virulent pathogen… for which there was no natural immunity… and no effective antivirals.” So we see that the official narrative was not only that SARS-CoV-2 was recently discovered, but that it did not exist before late December 2019, was different from other viruses, was newly capable of infecting humans, was entirely new to our immune system, and was outside the scope of what doctors knew how to treat.
Are any of these claims true? Other than the fact that it was recently identified, the other claims are either false or dubious at best. It is useful to examine each claim on its own. We begin with a brief investigation into the possibility that SARS-CoV-2 existed before December 2019. Actually, there is growing evidence that SARS-CoV-2 was around long before it suddenly acquired international attention. For instance, by searching through the public sequencing data archives, a group of researchers found that soil samples collected in Antarctica between Dec 2018 and Jan 2019 contained “sequence fragments matching the SARS-CoV-2 reference genome….” [9] This was so contrary to the official narrative that the authors later suggested that it had to be on account of laboratory contamination issues. But their findings were not unique. For example, by examining human blood samples taken in Italy before the Covid era, researchers found that already by September of 2019 some individuals (none of whom were sick at the time) had SARS-CoV-2 specific antibodies in their blood.[10 11] Other studies have found similarly.[12] Therefore, there is good evidence that the virus existed long before it garnered any attention.
Second, was SARS-CoV-2 that different from other viruses? The very fact that the virus was named “SARS-CoV-2” informs us that virologists think it is similar enough to SARS that it didn’t even warrant an entirely new name. Indeed, the two viruses are said to share “79.5% sequence identity.” [13] Despite the 20.5% difference, and notwithstanding the 17 year time lapse, studies have shown that people that were infected with SARS “possess long-lasting memory T cells…that displayed robust cross-reactivity to the N-protein of SARS-CoV-2.”[14] Therefore, although possessing differences, it cannot be said that this virus is that different from other coronaviruses.
Third, was this virus newly capable of infecting humans? To answer this question, it may help to consider RaTG13, a bat coronavirus that is said to be the closest to our virus. The two viruses are reported to be 96% similar.[15] Although it is commonly assumed that bat coronaviruses cannot infect humans without either a modification to its RNA or via an intermediate host, it is possible that bat coronaviruses jump to humans all the time, only without making us sick. For instance, a study done in 2018 found good evidence to conclude that bat coronaviruses are capable of infecting humans regularly, noting also that the “infections were subclinical or caused only mild symptoms.” [16] Conversely, experiments with blood samples of health care workers known to have had Covid demonstrated efficient neutralization of RaTG13.[15] Of particular significance in this regard is the little known fact that the PCR test for Covid, as designed by Drosten, was initially verified by making sure it detected coronaviruses from “bats in Europe and Asia.”[17] In other words, a positive PCR test may have indicated nothing more or less than the presence of a harmless bat coronavirus already endemic among humans. Although the Drosten test was later superseded by other tests, the official narrative emerged rapidly out of case detection using the Drosten test. Unfortunately, it is not clear to what extent this influenced early test results. In any case, it is certainly not novel that a virus of this sort could infect humans.
Fourth, is this virus entirely new to our immune system? Certainly not, for it was known from early on in the Covid-era that a significant percentage of people were immune to this supposedly novel virus. We previously observed that only 19% (712 of 3711) of the people on board the Diamond Princess cruise ship tested positive for the virus, and of these only a smaller fraction yet actually became ill.[4] Similarly, a group of researchers from Singapore “detected SARS-CoV-2 specific T cells in individuals with no history of SARS [or] Covid-19.” Remarkably, they also detected T cells in people that had no known contact with anyone that had had either SARS or Covid.[14] Likewise, a study in the UK found that many health care workers repeatedly tested negative despite repeated exposure to Covid.[18] The authors of that study concluded that “some individuals may clear subclinical infection before seroconversion.” Why did so many people never get Covid? Multiple researchers have concluded that it was likely a result of memory T-cells from a previous infection with a common cold or flu.[19, 20, 21, 22]
What percentage of people had sufficient prior immunity to prevent illness? Those same researchers found it was about 50%. For instance, a study by Grifoni et al “detected SARS-CoV-2-reactive CD4+ T cells in ~ 40% – 60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.” [23] In other words, about half the population was destined to never become noticeably ill from Covid for the simple reason that they recently had a cold. Nor is this particularly surprising since it was known that the original SARS virus had also cross-reacted with other coronaviruses.[24] Thus, the virus was not entirely novel to our immune system.
Fifth, was this virus new to doctors? As may be gathered from the fact that Covid was around long before March 2020, it is almost certain that before doctors were told that they were dealing with a novel virus that they supposedly did not know how to treat, they must have unknowingly treated Covid as if it was any normal respiratory or influenza-like-illness. To the best of our knowledge, there is no record of doctors reporting an unusual increase in untreatable respiratory disease, at least not until the WHO officially declared Covid a pandemic. Even after doctors were advised it was an entirely new disease, treatment protocols were rapidly developed in multiple places.[25, 26, 27]
In summary, SARS-CoV-2 was “novel” only in the sense that it was first discovered in early 2020. It is certain that it existed globally for at least six months before this. Already by January 2020 about half the world’s population was immune to this virus. Nor was Covid outside the parameters of known treatments available for respiratory diseases. These facts should have been front and center in the media, and should have had a strong influence on government policies. Sadly, all this information was buried.
Of course, if Covid was not novel, it is impossible that it should have caused any excess deaths in 2020. It follows from this sobering conclusion that any and all excess deaths had to have been caused by other factors.
2. How deadly was Covid?
As was just pointed out, at least half of the population was essentially immune to Covid. For these people Covid was a non-issue. What about the other half? How lethal was it for them? Central to a proper answer of this question is the fact that our immune system is confronted with novel proteins all the time. Our survival does not depend on us having seen them or anything similar before. Rather, the immune system learns from all foreign material, remembers the experience, and serves to make future encounters less noteworthy. If at some point in the future a virus should arise that was both novel to our immune system and untreatable, even this would not necessarily mean that the virus was something to fear; certainly not to the extent of causing a cataclysm like we have recently witnessed.
In a previous article of this series [1] we made mention of a World Health Organization bulletin that estimated the Infection Fatality Rate (IFR) of Covid to be 0.23%.[28] That same bulletin also advised it might be substantially less than this. As data accumulated, the IFR was indeed found to be lower, eventually converging on a global average of about 0.15%.[29] For people under 70 years old, the average IFR of Covid drops down to 0.07%.[30] Of course these estimates were determined using information from death certificates and PCR test results, which (as shall be explained below) may have introduced significant inflationary errors into the results. The IFR of Covid may therefore be much less than 0.15%.
Moreover, it is well established that severe Covid illness is generally linked to those with underlying medical conditions, meaning it is rare in healthy individuals. For instance, a study looking at more than half a million people hospitalized in the USA with Covid found that 94.9% “had at least 1 underlying medical condition.” [31]
Nevertheless, for the sake of argument let us accept these estimates at face value and proceed to ask how Covid compares with the flu? The IFR of influenza is generally considered to be about 0.1%, and in a typical season about 8% of Americans get sick from the flu.[32] As for Covid, despite the unprecedented numbers of people that were tested for this virus, the total number of Covid cases in the USA during 2020 totaled 19.2 million,[33] or about 5.7% of the population. Thus, by all metrics it would appear that Covid in 2020 was on par with or less than a normal flu season.
The fact that Covid is not a particularly lethal disease was known since early 2020. For instance, the UK government officially declared that “as of 19 March 2020, Covid-19 is no longer considered to be an HCID in the UK.” [34] The acronym HCID stands for “high consequence infectious diseases.” Therefore, for the vast majority of people, the wonderful and immensely complicated human immune system was more than adequate to fight off a Covid infection.
If in fact Covid was only as bad as a normal flu season, why did it garner so much attention? And why have government dashboards suggested that Covid is causing millions of excess deaths in the world? The answer to the first of these two questions will have to be postponed for a future article. As for the second question, it is helpful to look a little closer at excess deaths in 2020. A recent study by Levitt et al analyzed all-cause mortality rates in 33 countries from 2009 to 2021.They found that during this 13 year window, the year 2020 was the worst year with the highest mortality for only four countries: “UK, Italy, Spain and Belgium.” [35] Another 10 countries had “the highest mortality in 2021.” (USA and Poland were the worst). As for the remaining 19 countries, either 2009 or 2010 had the highest mortality.
Was there anything particularly special about 2009 that made it the worst year for more than half these countries? Actually, it was found to be the worst for two simple reasons: mortality rates have in general been decreasing over time, and 2009 is as far back as the study went. Of interest is that in 2009 the WHO declared a pandemic on account of the H1N1 virus. Nothing special came of it, however, for “the total number of influenza-related deaths worldwide… proved similar to the number in a relatively mild year of seasonal influenza.” [36]
The fact that 2020 was the worst year for only 4 of these 33 countries lends support to our conclusion that Covid was about as bad as a normal flu season. The fact that 2021 was the worst year for 10 countries helps reinforce our previous findings that the Covid shots did very little to prevent Covid deaths and instead caused a great deal of deaths from adverse events.
3. Covid Data Issues
How is it possible that a mortality analysis seems to contradict reports about millions of Covid cases and deaths? There are several good reasons for this apparent discrepancy. For starters, and as was mentioned in a previous article,[1] on April 20, 2020 the WHO mandated changes to the way death certificates were to be filled out. The document stated that “a death due to Covid-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness.” [37] In other words, since influenza typically has identical symptoms to Covid, flu deaths were to be labeled as Covid deaths. While this may be useful for “surveillance purposes,” it does not help us determine if Covid caused any excess deaths. Nor is it useful for making accurate comparisons between Covid and the flu. And it most definitely makes it difficult to calculate the IFR of Covid.
The WHO document went on to say: “A death due to Covid-19 may not be attributed to another disease (e.g. cancer)…. Always apply these instructions whether they can be considered medically correct or not.” Therefore, even if cancer was the actual cause of death, if the person so much as tested positive for Covid, the death certificate was to say that Covid was the cause of death. The end result of this change in policy is that the number of deaths caused by Covid has been significantly over-counted in most countries.[38, 39, 40, 41] What was not affected by the protocol change was how many people died from all causes. This is why all-cause mortality studies are so relevant during the Covid-era.
Another issue muddying the waters is the PCR test used to identify a Covid case. Despite the fact that the PCR test is based on remarkable technology, it has various shortcomings when used as it was to establish a Covid case. Very briefly, a few such issues are:
- If the cycle threshold is too high, it will return a high number of false positives.[42]
- As disease prevalence decreases, the risk of false positives increases.[43, 44]
- The number and type of primers used for identifying the presence of SARS-CoV-2 has the potential to pick up fragments originating from some other source.[45, 46] (As we saw above, harmless bat coronaviruses may give a false positive.)
- The PCR test is capable of finding virus fragments,or intact virus in the airway, but is not capable of determining if a person is actually infected with Covid. Since clinical symptoms were not required to be present, many uninfected individuals falsely tested positive. [47, 48]
Every issue listed above has the tendency to inflate Covid deaths.
4. Covid in Canada
To put things into perspective, and to tie all these ideas together, it is appropriate to consider one particular country in more detail as an example. Let us consider Canada. Statistics Canada records that 16,151 deaths in 2020 were attributed to Covid.[49] This is slightly more than twice the number of deaths attributed to “Influenza and Pneumonia” in an average year in Canada (7304 deaths/yr). How is it possible that Covid was more than twice as deadly as the flu if the two illnesses are about the same?
The answer is either that the number of Covid deaths was overcounted due to all the issues just mentioned or that influenza deaths were underdiagnosed in the past. Unfortunately, it is now nearly impossible to determine the exact error rate. Nevertheless, by considering only the last of the issues in the above list, it is possible to demonstrate how significant the inflation factor really is.
Dr. Bullard, head of the provincial laboratory in Winnipeg Manitoba, testified that PCR tests do not verify infection and were never intended to be used to diagnose respiratory illness.[50] He went on to say that about 56% of positives in Canada belonged to people that were not infected with Covid. If we accept this percentage, in all likelihood at least 56% of the deaths attributed to Covid in Canada were a result of a false positive. Applying this error rate to Covid deaths in Canada in 2020 brings the number of deaths down to 7,106. It is duly noted that this number is slightly lower than the yearly average for influenza deaths in the preceding four years. If we use this adjusted amount, and plot mortality in Canada in 2020 by the top 15 leading causes of death, we can see the relative significance of Covid in Canada.
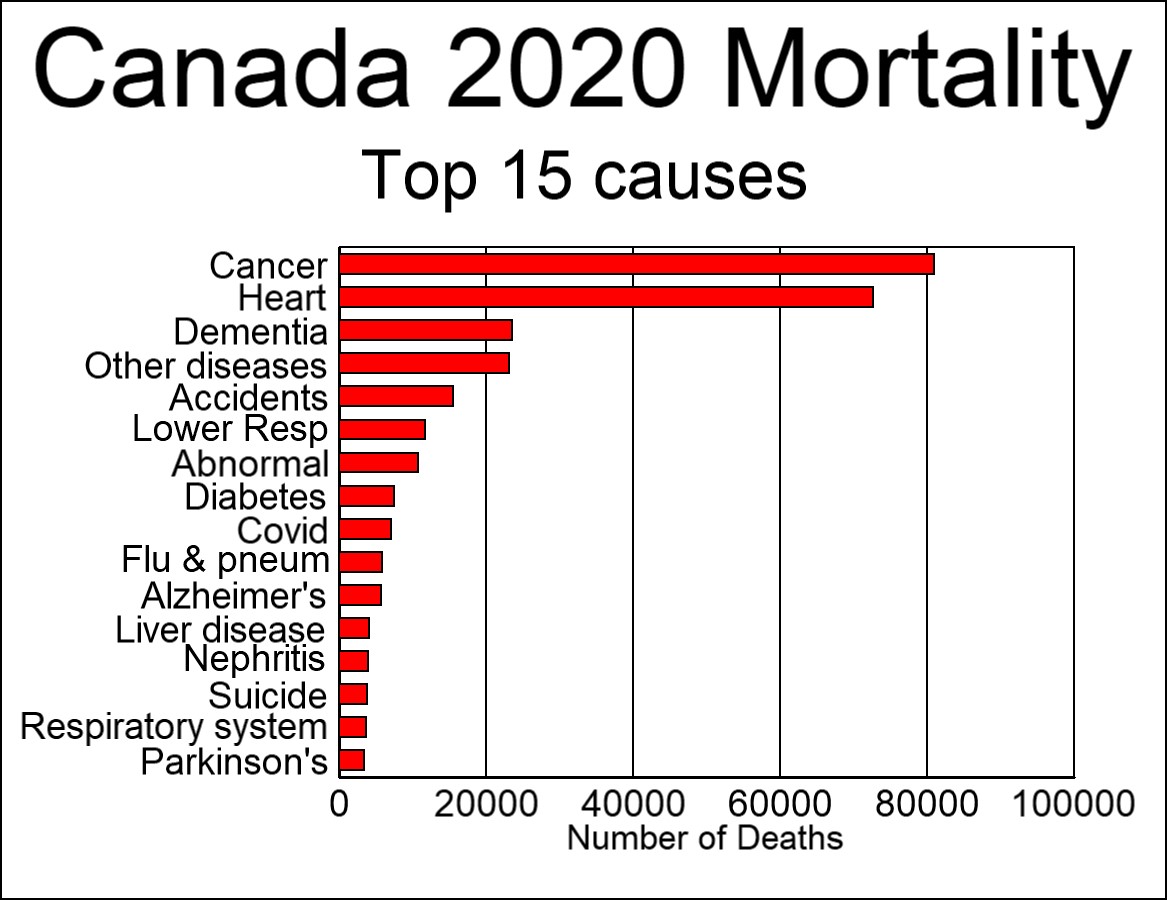
Covid mortality was adjusted down by 56% to account for false positives.
In Figure 1 above, cancer and heart issues dwarf all other causes of death. The number of deaths attributed to flu and pneumonia is several thousand below average. This resulted from the fact that, according to the WHO mandate, many deaths that would normally have been classified as influenza were labeled as Covid because the two are clinically compatible illnesses. Also, Canadian labs changed the way they tested for the flu: “changes in laboratory testing practices as a result of the public health response to… Covid-19… may affect the comparability of data to previous… seasons.” [51] What is clear from this chart is that Covid was not particularly lethal, was no worse than a normal flu season, and certainly unworthy of the unprecedented attention it received.
Conclusion
In conclusion, it is safe to say that SARS-CoV-2 was “novel” in early 2020 solely because of the simple fact that that is when it was first detected. Not only was Covid treatable, but at least 50% of people had sufficient immunity from a previous common cold to prevent noticeable illness. It can also be said that Covid was not unusually lethal, since the mortality burden was only as bad as a normal flu season. Covid mortality (when adjusted for only one of several factors) ranked ninth among the leading causes of death in Canada, the same rank normally held by influenza and pneumonia.
Of course, it could be argued that the reason Covid deaths were this low is because government mandated lockdowns and other non-pharmaceutical interventions prevented a Covid catastrophe. It is this important topic that we plan to cover in our next article of this series.
References
- Kenyon, Todd et al, “It is impossible that the vaccines saved 14 million lives in 2021,” Panda, 2023, https://pandata.org/drivers-of-excess-deaths-part1/
- Verduyn et al, “How many lives were actually saved by the Covid-19 vaccines?” Panda, 2023, https://pandata.org/how-many-lives-were-actually-saved-by-the-covid-19-vaccines/
- Kenyon, Todd et al, “What the Diamond Princess tells us about NYC in spring 2020,” Panda, 2023, https://pandata.org/what-the-diamond-princess-tells-us-about-nyc-in-spring-2020/
- Verduyn, Thomas et al, “Did side effects from the Covid shots cause an excess mortality?” Panda, 2023, https://pandata.org/did-side-effects-from-the-covid-shots-cause-any-excess-mortality/
- Akronson, Jeffrey, “Covid-19: First coronavirus was described in The BMJ in 1965,” BMJ 2020;369:m1547
- Mulley, Kary, US Patent, 1987, http://patentimages.storage.googleapis.com/cc/f0/3e/dc51b1fb4af2e6/US4683202.pdf
- Morris, Dylan, “Novelty Means Severity: The Key To the Pandemic,” Insight, 2021, https://www.theinsight.org/p/novelty-means-severity-the-key-to
- Billingsley, Alyssa, Pinto-Garcia, Patricia, “The Novel Coronavirus: What Are Novel Viruses, and How Do They Impact Public Health?” GoodRx Health, 2023, https://www.goodrx.com/conditions/covid-19/what-does-novel-coronavirus-mean-science-medical-definition
- István Csabai, Krisztián Papp, Dávid Visontai et al. “Unique SARS-CoV-2 variant found in public sequence data of Antarctic soil samples collected in 2018-2019,” 23 December 2021, PREPRINT (Version 1) available at Research Square https://doi.org/10.21203/rs.3.rs-1177047/v1
- Apolone G, Montomoli E, Manenti A, et al. “Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy.” Tumori Journal. 2021;107(5):446-451. doi:10.1177/0300891620974755
- Antonella Amendola, et al, “Molecular evidence for SARS-CoV-2 in samples collected from patients with morbilliform eruptions since late 2019 in Lombardy, northern Italy,” Environmental Research, Volume 215, Part 1, 2022, 113979,ISSN 0013-9351, https://www.sciencedirect.com/science/article/pii/S0013935122013068
- Jones, Will, “The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019,” 2022, The Daily Sceptic, The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019 – The Daily Sceptic
- Rossi GA, Sacco O, Mancino E, Cristiani L, Midulla F. “Differences and similarities between SARS-CoV and SARS-CoV-2: spike receptor-binding domain recognition and host cell infection with support of cellular serine proteases.” Infection. 2020 Oct;48(5):665-669. doi: 10.1007/s15010-020-01486-5. Epub 2020 Jul 31. PMID: 32737833; PMCID: PMC7393809
- Le Bert, N., Tan, A.T., Kunasegaran, K. et al. “SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls.” Nature 584, 457–462 (2020). https://doi.org/10.1038/s41586-020-2550-z
- Cantoni, D., Mayora-Neto, M., Thakur, N. et al. “Pseudotyped Bat Coronavirus RaTG13 is efficiently neutralised by convalescent sera from SARS-CoV-2 infected patients.” Commun Biol 5, 409 (2022). https://doi.org/10.1038/s42003-022-03325-9
- Wang, N., Li, SY., Yang, XL. et al. “Serological Evidence of Bat SARS-Related Coronavirus Infection in Humans, China.” Virol. Sin. 33, 104–107 (2018). https://doi.org/10.1007/s12250-018-0012-7
- Corman, Victor M et al, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR,” Eurosurveillance, 25, 2000045 (2020), https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045
- Swadling, L., Diniz, M.O., Schmidt, N.M. et al. “Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2.” Nature 601, 110–117 (2022). https://doi.org/10.1038/s41586-021-04186-8
- Jose Mateus et al., “Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans.” Science, 370,89-94(2020). DOI:10.1126/science.abd3871
- Lipsitch, M., Grad, Y.H., Sette, A. et al. “Cross-reactive memory T cells and herd immunity to SARS-CoV-2.” Nat Rev Immunol 20, 709–713 (2020). https://doi.org/10.1038/s41577-020-00460-4
- Humbert, Marion et al, “Functional SARS-CoV-2 cross-reactive CD4+ T cells established in early childhood decline with age,” PNAS, 2023, https://doi.org/10.1073/pnas.2220320120
- Mahajan, S., Kode, V., Bhojak, K. et al. “Immunodominant T-cell epitopes from the SARS-CoV-2 spike antigen reveal robust pre-existing T-cell immunity in unexposed individuals.” Sci Rep 11, 13164 (2021). https://doi.org/10.1038/s41598-021-92521-4
- Grifoni, Alba et al, “Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals,” Cell, 2020, DOI:https://doi.org/10.1016/j.cell.2020.05.015
- Patrick, David et al, “An Outbreak of Human Coronavirus OC43 Infection and Serological Cross-Reactivity with SARS Coronavirus,” Canadian Journal of Infectious Diseases and Medical Microbiology, 2006, https://doi.org/10.1155/2006/152612
- Front Line Covid Critical Care Alliance, Treatment Protocol, https://covid19criticalcare.com/treatment-protocols/
- Heart Advisory & Recovery Team, Ivermectin, https://www.hartgroup.org/category/ivermectin/
- McCullough PA, et al, “Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19).” Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264. PMID: 33387997.
- Ioannidis, John P A. (2021). “Infection fatality rate of COVID-19 inferred from seroprevalence data.” Bulletin of the World Health Organization, 99 (1), 19 – 33F. World Health Organization. http://dx.doi.org/10.2471/BLT.20.265892
- Ioannidis, John P A. “Reconciling estimates of global spread and infection fatality rates of COVID-19: An overview of systematic evaluations,” European Journal of Clinical Investigation, 2021, https://doi.org/10.1111/eci.13554
- Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. “Age-stratified infection fatality rate of COVID-19 in the non-elderly population.” Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797.
- Kompaniyets, Lyudmyla et al, “Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020–March 2021,” CDC 2021, DOI: http://dx.doi.org/10.5888/pcd18.210123external icon
- Anonymous, “Key Facts About Influenza (Flu),” CDC 2022, https://www.cdc.gov/flu/about/keyfacts.htm
- Anonymous, Our World In Data, Coronavirus (COVID-19) Cases – Our World in Data
- Anonymous, “Guidance High consequence infectious diseases (HCID),” UK government, 2020, https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid
- Levitt, M., Zonta, F. & Ioannidis, J.P.A. “Excess death estimates from multiverse analysis in 2009–2021.” Eur J Epidemiol (2023). https://doi.org/10.1007/s10654-023-00998-2
- Fineberg, Harvey, “Pandemic Preparedness and Response — Lessons from the H1N1 Influenza of 2009,” N Engl J Med 2014; 370:1335-1342 DOI: 10.1056/NEJMra1208802
- Anonymous, “International Guidelines for Certification and Classification (coding) of Covid-19 as Cause of Death,” World Health Organization, 2020, https://cdn.who.int/media/docs/default-source/classification/icd/covid-19/guidelines-cause-of-death-covid-19-20200420-en.pdf (pg 3)
- Audie, Joseph, “Using CDC data and death certificate standards to propose a preliminary estimate for the number of US COVID-19 associated deaths that were caused by or contributed to by SARS-CoV-2 infection,” Research Gate, 2020, https://www.researchgate.net/publication/344228032_Using_CDC_data_and_death_certificate_standards_to_propose_a_preliminary_estimate_for_the_number_of_US_COVID-19_associated_deaths_that_were_caused_by_or_contributed_to_by_SARS-CoV-2_infection
- Fenton, Norman & Neil, Martin & McLachlan, Scott. (2021). What proportion of people with COVID-19 do not get symptoms?. 10.13140/RG.2.2.33939.60968.
- Jensen, Scott, 2023, https://www.youtube.com/watch?app=desktop&v=PHxj_Luclxs&feature=youtu.be
- Beaudoin, John, “500,000 Death Certificates Tell of Signals, Fraud, and Unlawful Deaths,” 2023, https://rumble.com/v2a7wtk-john-beaudoin-500000-death-certificates-tell-of-signals-fraud-and-unlawful-.html
- La Scola B, Le Bideau M, Andreani J, Hoang VT, Grimaldier C, Colson P, Gautret P, Raoult D. “Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards.” Eur J Clin Microbiol Infect Dis. 2020 Jun;39(6):1059-1061. doi: 10.1007/s10096-020-03913-9. Epub 2020 Apr 27. PMID: 32342252; PMCID: PMC7185831.
- Anonymous, “WHO Information Notice for Users 2020/05: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2,” World Health Organization, 2021, https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
- Deeks, John, “Why the school testing regime needs to change,” The Post, 2021, https://unherd.com/thepost/why-the-school-testing-regime-needs-to-change/
- Neil, Martin, “Put to the test: use of rapid testing technologies for covid-19,” BMJ 2021; 372 doi: https://doi.org/10.1136/bmj.n208
- Neil, Martin, “UK lighthouse laboratories testing for SARS-COV-2 may have breached WHO Emergency Use Assessment and potentially violated Manufacturer Instructions for Use.” Probability and Risk, 2021, https://probabilityandlaw.blogspot.com/2021/02/uk-lighthouse-laboratories-testing-for.html?m=1
- Deeks, Jonathan, “Operation Moonshot proposals are scientifically unsound,” BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m3699
- Pollock A M, Lancaster J. “Asymptomatic transmission of covid-19” BMJ 2020; 371 :m4851 doi:10.1136/bmj.m4851
- Anonymous, Statistics Canada. Table 13-10-0392-01 “Deaths and age-specific mortality rates, by selected grouped causes” DOI: https://doi.org/10.25318/1310039201-eng
- Anonymous, “Manitoba Chief Microbiologist and Laboratory Specialist: 56% of positive “cases” are not infectious,” JCCF, 2021, https://www.jccf.ca/manitoba-chief-microbiologist-and-laboratory-specialist-56-of-positive-cases-are-not-infectious/
- Government of Canada, “FluWatch annual report: 2019-2020 influenza season,” 2021, https://www.canada.ca/en/public-health/services/publications/diseases-conditions/fluwatch/2019-2020/annual-report.html
Disclaimer
Some of the posts we share are controversial and we do not necessarily agree with them in the whole extend. Sometimes we agree with the content or part of it but we do not agree with the narration or language. Nevertheless we find them somehow interesting, valuable and/or informative or we share them, because we strongly believe in freedom of speech, free press and journalism. We strongly encourage you to have a critical approach to all the content, do your own research and analysis to build your own opinion.
We would be glad to have your feedback.

Source: PANDA Read the original article here: https://pandata.org/