

Billions of dollars spent every year
Searching for a cure for cancer
Why not spend that money instead
To wipe out pollution that causes the cancerThrough DNA analysis
We may one day conquer disease
A “perfect” baby every time
By mapping and manipulating people’s genesLife insurance? Be serious!
You have to get your genes screened first
Toxic chemicals? Fumes at work?
No sweat! Get a gene transplant
Otherwise you’ll lose your job
You wanna wind up out in the streets?
And raise your children in campgrounds and shelters?
And beg to eatGerm warfare, more bombs
Germ warfare, more bombs
Our whole economy’s based on fear and death
How long can we get away with this?Wrong people, right place
Ruling class gets the only pass
To board the ark for outer spaceIn 2030, what about this place?
Jello Biafra and NOMEANSNO lyrics. The Sky is Falling and I Want My Mommy. 1991
I was meant to talk for about 15 minutes at a recent Brownstone retreat and found myself hovering my figurative mouse over the subject matter of cancer gene therapy for about 5 minutes instead. I thought it was important. In January 2024, the Lancet wrote up a study entitled “Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): a randomised, Phase 2b study” which was a summary of the phase 2 trial data for this ‘new’ product. You can read about that here, and here is the clinical trial study description at clinical trials dot gov NCT03897881.
Currently, we are moving into phase 3, and before you know it, everyone will be getting injected with modified mRNA crap to ‘cure cancer.’ Now don’t get me wrong, cancer is insidious and needs to be dealt with, but as I stated in my 5-minute short, cancer is almost entirely preventable (in the case of most cancers) and thus, resources should be spent on prevention, not Stage 4 ‘cures’ based on novel gene-based pro-drugs that have a really bad safety profile as per the Covid-19 modified mRNA injectable product test run of late.
On the 26th of April 2024, Sky News wrote up an article summarizing the ‘great news’ about this new ‘cure.’ They entitled it: “World’s first jab to stop skin cancer being tested in UK patients.” It is interesting to me that there is no mention of modified mRNA, and it is annoying to me that they refer to people as patients. I hate that. We’re not patients until we are at the hands of a doctor/medical facility. It’s almost as if they are priming us for life in the ‘new world’ where we will all be born as patients.
This ‘cure’ or therapy, if you will, is based on a concept called Individualized Neoantigen Therapy (INT), which in and of itself, is a genius concept, however unnecessary. Since this therapy is based on the now ‘traditional’ Covid-19 product lipid nanoparticle (LNP) platform, it is inherently dangerous, in my opinion.
An antigen is a molecule that is able to have an antibody generated against it. Neoantigens are tumour-specific and produced by cancer cells. Cancer cells have their basis in specific and cumulative DNA mutations that result in the production of neoantigens. Neo comes from the Greek neos that means ‘new’, so these neoantigens are simply new antigens (tumor-specific) not yet seen by the immune system.
The idea in the phase 2 clinical trial thus far, is that melanoma cancers can be biopsied, the DNA therein deep-sequenced, and the DNA of personalized neoantigens associated with the tumor discovered. With these in hand, a targeted offense against the specific cancer cells can be made.
Used in conjunction with pembrolizumab, they claim that cancer recurrence was reduced when compared to only pembrolizumab use. This clinical trial began in July 2019 and the first submission was made in March 2019. Funny that.
The mRNA stuff used as the payload even has a Wikipedia page. Look for mRNA-4157/V940. As mentioned, the delivery vehicle are the LNPs that as we all well know now, are made with highly-charged cationic lipids – the same ones that are known to have high toxicity profiles in humans. The same ones used to deliver the modified mRNA used in the Covid shots.
These LNPs STILL have no study associated with their use in the absence of payload, as far as I am aware. I believe that beyond the toxicity of the cationic lipids, these LNPs are notoriously hazardous based on their potential ability to disrupt the zeta potential of red blood cells. We only hypothetically know what their zeta potential is in the context of the Covid products – it is meant to be 3.13 mV – but is it? Do they even have a neutral zeta potential?
I like this article written by Sarah Whelan for Technology Networks explaining what neoantigens are, how they arise, and how the ‘cancer therapy’ may work in their context. She goes into the differences between individualized and shared neoantigens in the context of cancer antigens.
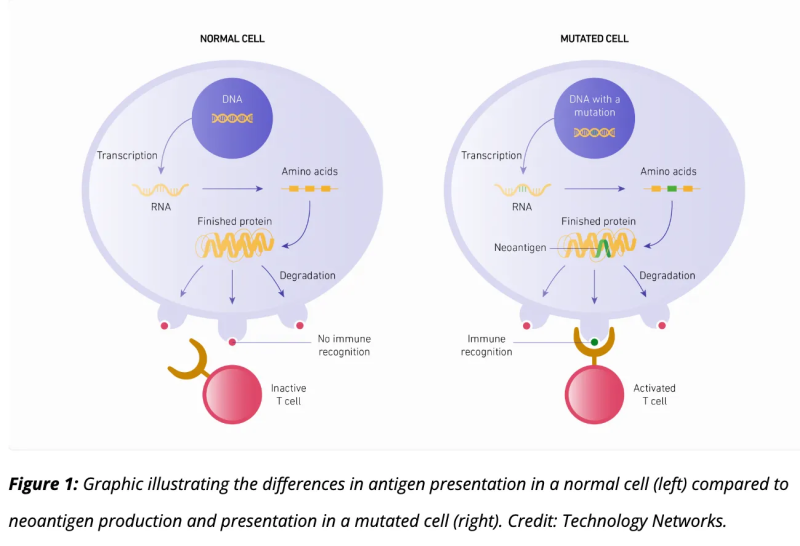
The gene-based therapy targets these specific antigens in the following way.
The modified mRNA payload in the LNPs – mRNA-4157 – is a sequence of nucleotides, just like for the spike protein, that encodes 34 identified neoantigens and upon transfection using the LNPs as trojan horses, the synthetic mRNA is translated by the host cell machinery into subsequent proteins. These proteins get chopped up once produced by inherent host cell enzymes, and mounted on MHC molecules as antigenic peptides on the outside of the cell. This is a part of normal intracellular antigen processing and in fact, the designed mechanism of action for this ‘therapy’. The T cells that can recognize the peptides presented on the MHC molecules will respond by killing the cell, if they are CTLs, for example. So the key here, in my opinion, is to target – very precisely – the cancer cells with the LNPs.
About mRNA-4157 (V940)
mRNA-4157 (V940) is a novel investigational messenger RNA (mRNA)-based individualized neoantigen therapy (INT) consisting of a synthetic mRNA coding for up to 34 neoantigens that is designed and produced based on the unique mutational signature of the DNA sequence of the patient’s tumor. Upon administration into the body, the algorithmically derived and RNA-encoded neoantigen sequences are endogenously translated and undergo natural cellular antigen processing and presentation, a key step in adaptive immunity. Individualized neoantigen therapies are designed to train and activate an antitumor immune response by generating specific T-cell responses based on the unique mutational signature of a patient’s tumor.
So what will work for me, would not work for you. It’s kind of cool, but I would never partake. I would need to know far more about the targeting process with regard to the tumor itself, and of course, some studies on the empty LNPs, please.
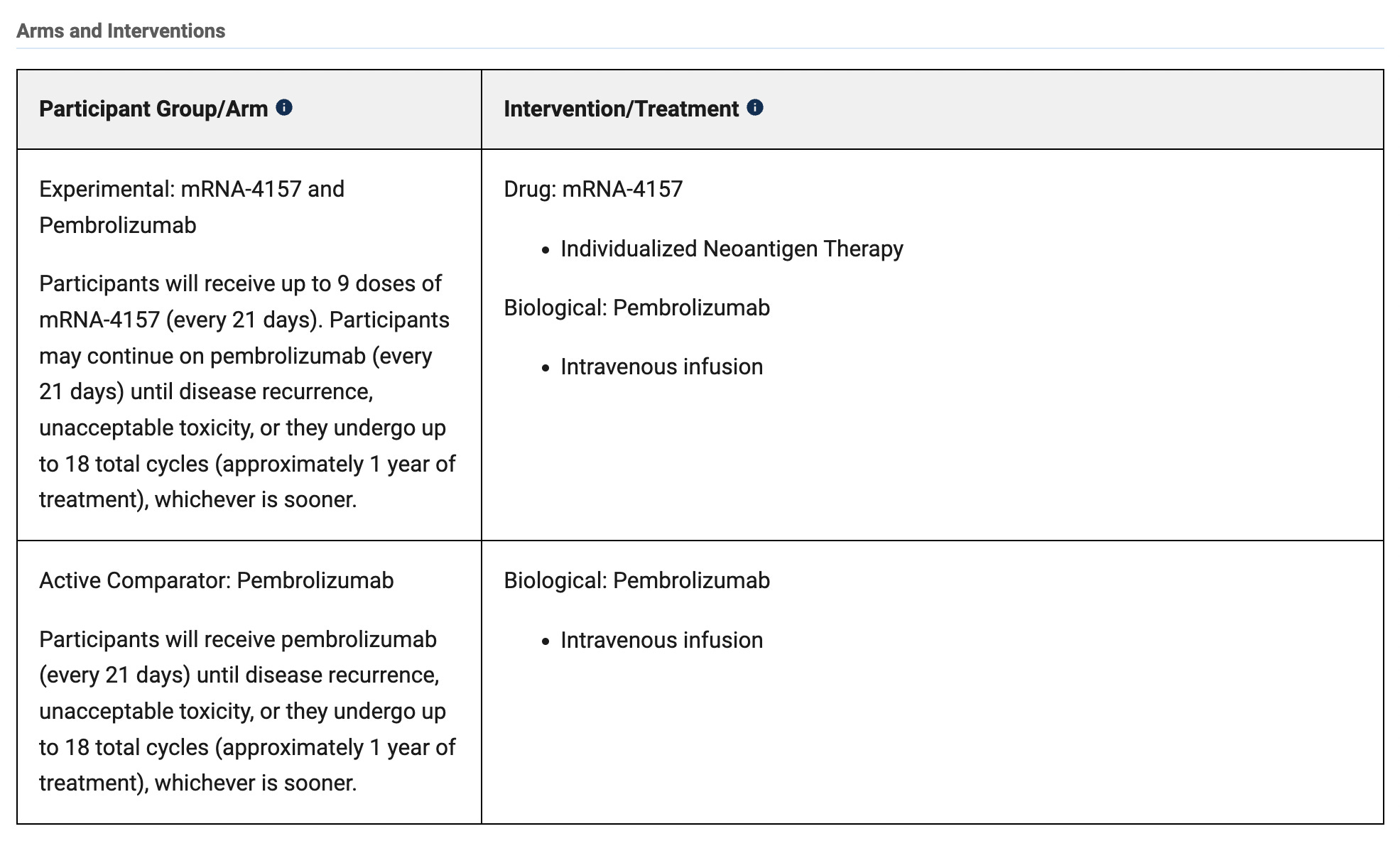
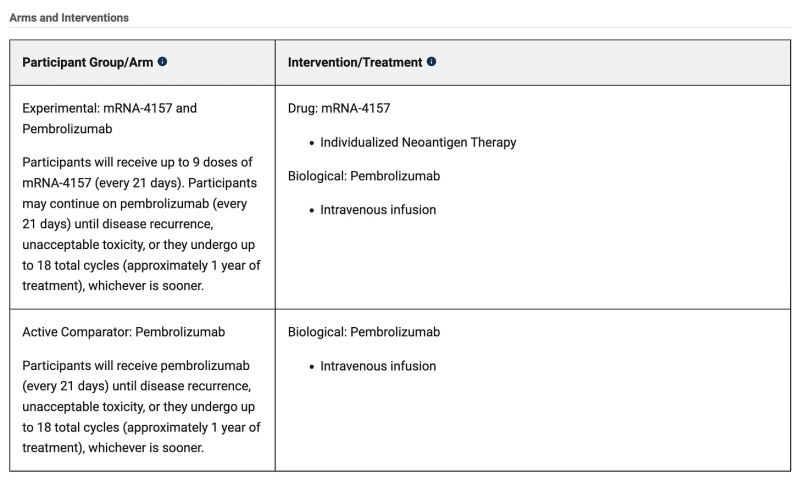
The NCT03897881 phase 2 clinical trial information (start date: 2019-07-18; end date: 2029-09-09) states that trial participants get up to 9 doses of the mRNA-4157 product every 21 days (dose-escalated) but it’s not clear how they are being administered. Are they local to the melanoma site? Are they intra-muscular like the Civud shots? They simply write “Individualized Neoantigen Therapy”. They do tell us that the pembrolizumab is an intravenous infusion.
{kind=link}
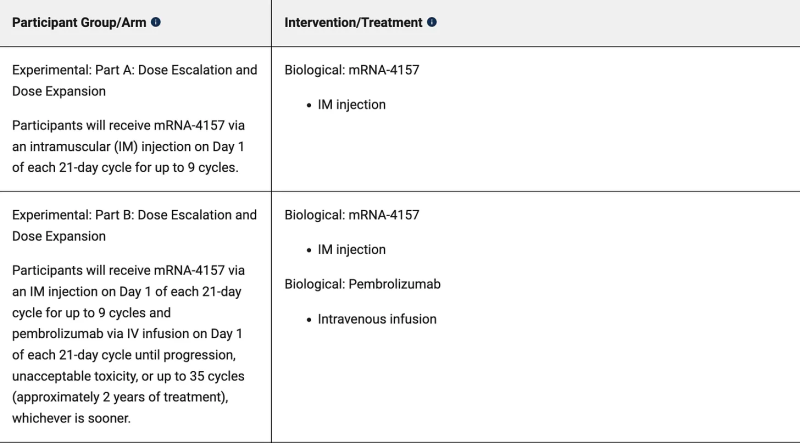
The NCT03313778 phase 1 clinical trial information (start date: 2017-08-14; end date: 2029-09-09) does state an intramuscular injection strategy. This is worrisome. Very worrisome. I would be correct in assuming that “Individualized Neoantigen Therapy” automatically means an intramuscular injection. I would be correct in assuming that this would be administered in the arm, just as the Covid shots were.
I would then be correct in assuming that the LNPs, unless designed for targeted administration, would go everywhere, as they did with the COVID LNPs. Wouldn’t this necessarily mean that random cells would get transfected and thus produce cancer neoantigens and mount them on their surfaces for specific killing?
{kind=link}
On the subject matter of specific LNPs, in one article I read in my research journey there was a mention of Onpattro, and if you’re up-to-date on my articles, you know that this is an LNP-based therapy that uses specific LNPs that target the liver using APOE proteins on the surfaces of the LNPs. My question for now is, are the LNPs used for delivery of the mRNA-4157 specific, and if so, how are they targeted and where are they specific for? Are they embedded with the neoantigens and if so, how would that work? I would assume there are no cognate receptors for the neoantigens.
To get the LNPs to the cells likely to have the specific DNA mutations associated with the melanoma, I would think it best to inject the LNPs at the resected (removed) melanoma site using a subcutaneous injection. But what do I know?
That’s all for now. Prepare for the common use of the words “cancer cure”, “personalized medicine”, and “gene therapy” as part of the new world order lexicon. They’re also going to normalize the CRISPR/Cas-9 system and instead of imprisoning guys like He Jiankui, they will give them Nobel prizes soon. Just watch.
Read every word of these lyrics written decades ago…
First the urine test – now this!
First the urine test – now this!
Why do all the best technological advances
Always wind up in the worst possible hands
Through DNA analysis
We may one day conquer disease
A “perfect” baby every time
By mapping and manipulating people’s genes
Cosmetic surgery before you’re born
Know in advance what you’ll die of
Everyone is useful and the same
Swimmers bred like horses for olympic teams
Life insurance? Be serious!
You have to get your genes screened first
Toxic chemicals? Fumes at work?
No sweat! Get a gene transplant
Otherwise you’ll lose your job
You wanna wind up out in the streets?
And raise your children in campgrounds and shelters?
And beg to eat
There’s too many sharks in the gene pool
Too many chewed up bodies on the shore
Too many sharks in the gene pool
Too many leftovers rotting all around usFirst the urine test – now this!
Why do the best technological advances
Keep winding up as…
Uniform hybrid species
For fresh-looking pest-proof food
An apple can sit on the shelf for years
When we irradiate the molecules
But where did the nutrition go?
And what’s taken it’s place?
Slipshod tampering with science
Out of control factory farm eugenics
Slaughterhouses in lowa
Filled with tumor-infested cows
Failed experiments hidden ’til sold
To your local school lunch program
Grade D, but edible
Our food, our life, our attitude
Suffocating in what we refuse to recycle
Time bombs fester in every town
Billions of dollars spent every year
Searching for a cure for cancer
Why not spend that money instead
To wipe out pollution that causes the cancerThere’s too many sharks in the gene pool
Too many screw-ups washing on shore
Too many sharks in the gene pool
Too many preventable accidents among us
Meryl Streep… where are you?
Where did American know how go
Why do Japanese build better stereos
Is it ‘cos our best minds can’t get a job?
Except when they help make toys for the Pentagon
Germ warfare, more bombs
Germ warfare, more bombs
Our whole economy’s based on fear and death
How long can we get away with this?
And we live here
Instead of better health we get AIDS
Instead of nourishment we get steroids
The most popular selections at celebrity sperm banks
Are sports heroes
Gap widens between the haves and the have-nots
Rich and powerful breed only with themselves
We all know what happens when too much of this happens
The offspring just ain’t real brightHow else can you explain
The erosion of talent and the vision thing
To the point where the best that they can come up with
For our future role models and leaders
Are vicious blind machines
Like Albert Gore and Dan Quayle
Why do the best solutions and advances
Get thrown away in the worst possible hands
There’s too many sharks in the gene pool
Too many carcasses washing on shore
Too many sharks in the gene pool
Avalanche of toxic guts all around us
We’re incompetent as human beings
Even worse at playing God
Wrong people, right place
Ruling class gets the only pass
To board the ark for outer space
In 2001, what about this place?
Republished from the author’s Substack
Disclaimer
Some of the posts we share are controversial and we do not necessarily agree with them in the whole extend. Sometimes we agree with the content or part of it but we do not agree with the narration or language. Nevertheless we find them somehow interesting, valuable and/or informative or we share them, because we strongly believe in freedom of speech, free press and journalism. We strongly encourage you to have a critical approach to all the content, do your own research and analysis to build your own opinion.
We would be glad to have your feedback.

Source: Brownstone Institute Read the original article here: https://brownstone.org/