

It’s interesting that the esteemed editor of this site has concluded, after more than four years of cogitation, that mRNA technology-based vaccines were a solution in search of a problem in the minds of a health-cum-national security elite, that SARS-CoV-2 was the answer to their prayers, and that lockdowns, masks, school restrictions, and rejection of alternative treatment options were necessary to prevent the achievement of herd immunity via infections before vaccines could be mass manufactured and rolled out to the whole world.
Unfortunately, Jeffrey Tucker points out, their preferred solution ‘failed spectacularly.’ Instead, what we have ‘unfolding here is the biggest and most destructive flop in the history of public health.’ Others go further, arguing that mRNA vaccines in particular have correlated so strongly with rising all-cause excess mortality that causation must be a strong presumption.
Yet, not everyone buys the overarching judgment of spectacular failure. The holdout proponents of the success of public health interventions point to the gravity and universality of the threat from Covid, on the one hand, and the public health benefits of the vaccines, on the other. On the first, for example, a year ago the World Health Organisation published estimates that in the two years 2020 and 2021, nearly 15 million people had died with Covid, or almost three times the official estimates.
A study published in the journal Lancet Infectious Disease in June 2022 estimated that Covid-19 vaccines saved 19.8 million lives in the first year of their availability, helping to reduce the global death toll by 63 percent. The study used a ‘mathematical model of Covid-19 transmission and vaccination.’ Another modeling study concluded that in two years, vaccines had saved around three million US lives. A paper by two US researchers in March this year, from the University of Colorado and University of California Los Angeles, calculated that 800,000 American lives were saved by lockdowns, social distancing, and vaccines.
A computer simulation modeling from Monash University in Melbourne estimated that vaccination prevented nearly 18,000 deaths in New South Wales alone in the one-year period from August 2021 to July 2022, reducing the death toll to one-sixth of what might have been expected otherwise. Unvaccinated 50-year-olds and over had twelve times higher mortality rates than their boosted counterparts.
These are tall claims, in both senses of the word. It’s impressive how many still try to bamboozle health reporters and the public with abstract mathematical models to claim spectacular success for Covid-19 vaccines. Assumptions are made about infection and case fatality rates and about the efficacy of vaccines to produce such favorable estimates. Several also assume that no immunity existed from natural infection at any point. Voluntary modifications of individual behavior to reduce risks as awareness of the pandemic spread is totally discounted. The variability in transmissibility and lethality of successive variants as the virus mutated is ignored.
The public health clerisy and vaccine manufacturers self-servingly classify everyone until two or three weeks after the second dose as ‘unvaccinated,’ when empirically the more useful binary data classification would be into the ever- and never-vaccinated.
There is the problem of coding errors in data collection, including wide variations in recording deaths as Covid-related. The difference between dying with and from Covid may well be impossible to disentangle by now. That doesn’t mean it is trivial. Covid as the sole or chief cause of death could amount to anything between 10-50 percent of the seven million total number of Covid-related deaths as of 21 May, as per Worldometers.
Then too, it is both indisputable and largely conceded by now that vaccine efficacy declines rapidly, and particularly so with successive booster doses, so that the date of data measurement also becomes critical. The healthy vaccinee effect is yet another confounding factor.
The most critical consideration is this: few studies promoting vaccines take care to separate the protection conferred by vaccines from that of naturally acquired immunity from prior infection. In a pithy summary on 20 May, Alex Berenson observed: ‘Science brought us an epidemic. Nature saved us.’
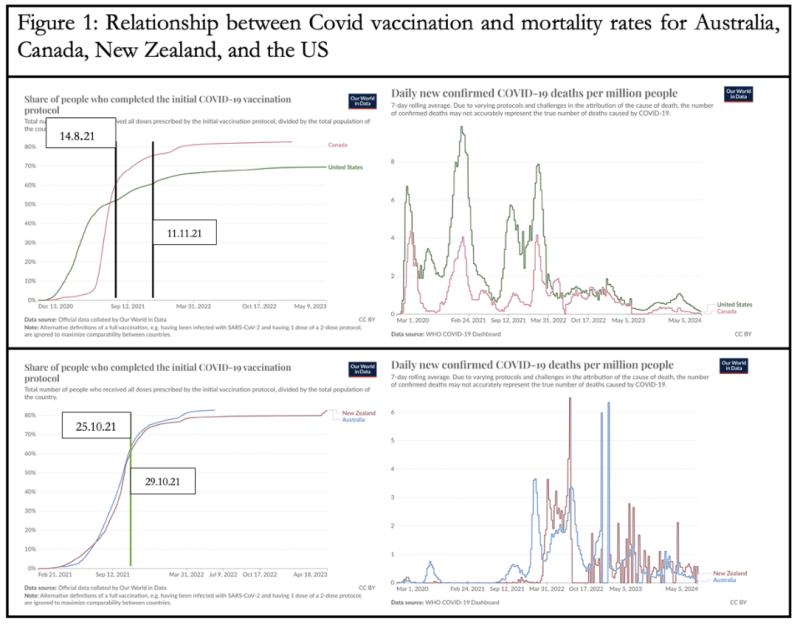
Consider two pairs of neighboring countries in the Northern and Southern Hemisphere: Canada and the US, and Australia and New Zealand (Figure 1). Because the US achieved 70 percent full (that is, two doses) vaccination quite late, I have chosen the arbitrary threshold of 60 percent for present comparative purposes. Canada and the US crossed the threshold in August and November 2021, while the Australasians did so in October.
Next, look at the dates on which the four countries recorded their highest daily mortality rates (7-day rolling averages) (Table 1). In the North American pair, well before getting to 60 percent vaccination; in Australasia, well after.

Note: unusually among the four countries under consideration, Canada experienced three broadly comparable peaks. The other two occurred on 28 January 2021, with a deaths per million rate of 4.05, and on 1 February 2022, 4.15 deaths per million people.
Canada hit 60 percent full vaccination on 14 August 2021, fifteen months after its peak daily Covid mortality rate and seven months after a mini-peak in January 2021. The United States hit 60 percent full vaccination on 11 November 2021, ten months after its highest daily Covid mortality rate. In other words, mortality rates had fallen in both these North American countries well before vaccination coverage got to 60 percent.
By contrast, Australia and New Zealand achieved 60 percent full vaccination on 25 and 29 October 2021, respectively and their Covid mortality peaked well afterwards: 16 months later for Australia and nine months later for New Zealand.
This is even better captured in the total number of cumulative Covid-related deaths.
For the United States, 63 percent of Covid-related deaths until May 2024 were recorded before 60 percent full vaccination, which is why public health and administration officials could not resist the temptation to conflate correlation and causation in the post-vaccination fall in deaths. This is less obvious for Canada, with 51.4 percent of its total deaths being recorded after 60 percent vaccination.
In Australia’s case, an astonishing 93 percent of the deaths were after 60 percent full vaccination. For New Zealand, the share is a staggering 99.3 percent. How anyone could claim this as vaccine success with a straight face is beyond comprehension. If correlation is to be posited as causation, therefore, clearly vaccines were driving Covid cases and deaths that had been remarkably low before vaccines began to be rolled out. But obviously, the same vaccines could not be driving Covid cases and mortality down in the US but causing a surge in Australasia.
In any case, even without equating correlation and causation, the two Australasian examples are sufficient to falsify the general claim of vaccine effectiveness. Unless, of course, the vaccine faithful would like to argue that there is some mysterious force that corrupts the vaccines as they cross the equator.
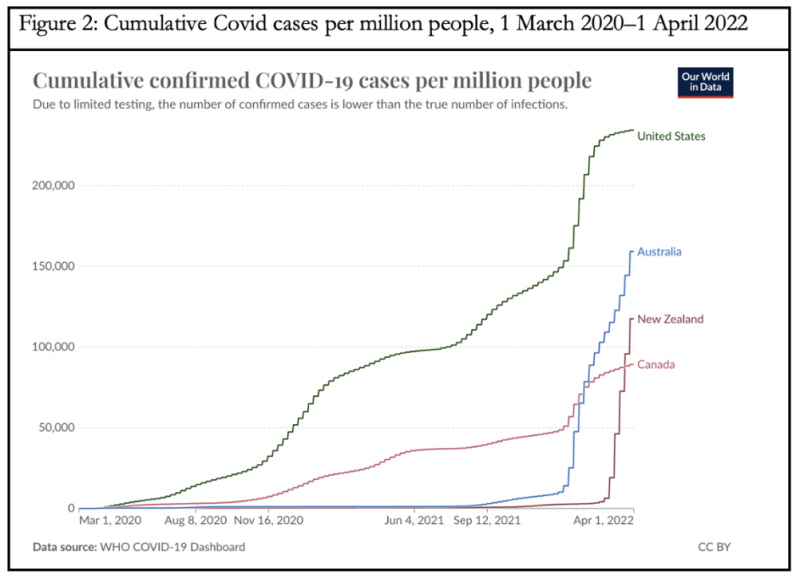
There is an alternative explanation that covers the four countries rather better. This points to the key role of natural immunity from prior infection. As shown in Figure 2, owing to the combination of summer in the Southern Hemisphere when the pandemic broke, geographical location, and international border closures, Australia and New Zealand succeeded in quarantining their populations from the virus for two years. As of 31 December 2021, the cumulative cases (defined as a positive test irrespective of feeling well or ill) per million people was 2,686 for New Zealand and 25,068 for Australia, but 56,907 for Canada and a whopping 161,373 for the United States. Thus huge numbers of Canadians and (especially) Americans had acquired natural immunity by then.
But this meant that over two years of isolation, unless the vaccines were highly efficacious and sustained their immunity for long timeframes, Australia and (especially) New Zealand had created immunologically naïve populations. Unless they intended to close off their borders to the outside world permanently, which was never even a possibility, their peoples were highly vulnerable to fresh waves of the virus once they reopened and until they acquired immunity that was both more robust and more durable.
In sum, therefore, looked at together, the two pairs of examples from North America and Australasia indicate a weak to negligible role of vaccines and the critical role of infection-acquired immunity in ending the pandemic. It’s called relearning the same lessons all over again.
Disclaimer
Some of the posts we share are controversial and we do not necessarily agree with them in the whole extend. Sometimes we agree with the content or part of it but we do not agree with the narration or language. Nevertheless we find them somehow interesting, valuable and/or informative or we share them, because we strongly believe in freedom of speech, free press and journalism. We strongly encourage you to have a critical approach to all the content, do your own research and analysis to build your own opinion.
We would be glad to have your feedback.

Source: Brownstone Institute Read the original article here: https://brownstone.org/