
[The following is an excerpt from Lori Weintz’s book, Mechanisms of Harm: Medicine in the Time of Covid-19.]
If you think about a virus, what’s the purpose? What’s the virus trying to do? It’s trying to stay alive…And if the virus kills someone, if it kills the host, it dies with the host. So it totally defeats the purpose.
Because the goal of a virus is to survive, replicate, and spread, it tends to evolve toward being more infectious and less deadly. There are exceptions and other factors, but in general…that’s what virologists expect to see occur with SARS-CoV-2, the coronavirus that causes COVID-19.
–Northeastern (University) Global News, December 13, 2021
In natural Covid infection, the virus enters the body through the nose and mouth. The spike protein of the virus binds with the ACE2 receptor in the nose and the virus replicates for a few days. The immune system either takes care of it there, or the virus continues into the lungs and a person becomes symptomatic while continuing to fight the infection.
For many people Covid has not been much more than a cold. Some have been completely asymptomatic. Others have had body aches and chills, fever, nasal stuffiness, nausea, cough, loss of taste and smell, exhaustion, and weakness, among other symptoms. Covid-19 can be a nasty disease, but from the beginning it had a 99.98% recovery rate, which means most people recover from Covid infection. The pattern for viruses is for them to become more transmissible, and less lethal. SARS-CoV-2 was no exception in this regard. With the advent of the Omicron variant, Covid became much milder than the original Wuhan and the Delta variants had been.
An important factor of natural Covid infection is the fact that those who recover from natural infection have immune systems trained to mount a response to all parts of the virus – not just the spike protein.
Severe Covid and the cytokine storms of Wuhan and Delta in 2020-2021:
The toxic part of the SARS-CoV-2 virus is the spike protein. For those unfortunate enough to experience severe Covid, the disease can progress to the point that the spike spreads through the bloodstream to the body’s organs, causing a cytokine storm. Cytokines are molecules that promote inflammation. In a cytokine storm, too many cytokines are released, leading to an over-activation of other immune cells such as T cells, macrophages (a type of white blood cell that helps eliminate pathogens), and natural killer cells. Essentially, in a cytokine storm, the immune system attacks the body it was meant to protect.
As the excess activity of these immune cells continues, damage occurs to the endothelial lining of the circulatory system and the alveoli of the lungs, and eventually leads to thrombosis, which involves blood clotting, circulation disorders and multiple organ failure.
Covid-19 is primarily a risk to the elderly and those with chronic illnesses:
Most people who contract Covid recover, even those who have some days of being very ill. Stanford professor John Ioannidis, a meta-research specialist, determined from early data that Covid-19 had a case fatality rate lower than influenza. (Ioannidis’ later meta-analysis, based on more data from around the world, placed the overall case fatality rate at 0.20 percent, but the figure was almost 0.0 percent for children and young people.)
Covid-19 disease has mostly impacted the elderly and those with other serious illnesses and conditions, such as diabetes and obesity. For example, in the U.S. over 80 percent of Covid deaths were in the 65 and older population, and almost all deaths, regardless of age, were in those with comorbidities. U.S. data in 2021, which held consistent in later evaluations, found that not one healthy child in the 0-12 age group died of Covid. In Sweden, where schools remained open throughout 2020 for primary and middle school students, there was not one Covid death among the 1.8 million children enrolled. (Sweden also did not mandate masks or social distancing in the schools, or other settings.)
Covid Wuhan and Delta variants were a serious disease for the vulnerable:
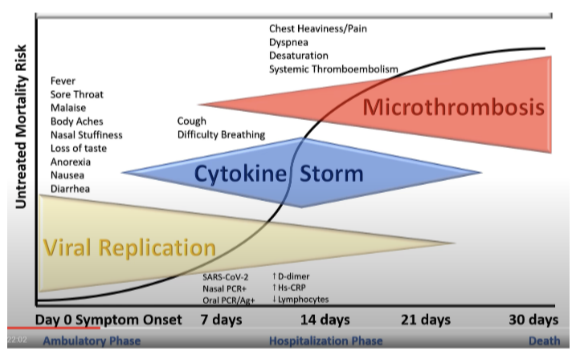
Because the original Wuhan variant and subsequent Delta variants of SARS-CoV-2 were more toxic, the failure to treat in early stages of the disease was an especially egregious lapse in medical ethics. The following chart released by cardiologist Dr. Peter McCullough in October 2020 shows the “Untreated Mortality Risk” in the stages of Covid-19 disease. The bar across the bottom shows the “Ambulatory Phase,” “Hospitalization Phase,” and “Death.” The black curved line shows the risk of mortality rising as the disease progresses without treatment.
I personally know of two people who died early in the Covid-19 pandemic because of failure to treat during the beginning viral replication phase of their illness. One was a neighbor, age 60, who was in good health when she contracted Covid. The other was the husband of an acquaintance, in his late 50s, who was slightly overweight and struggled during cold and flu season each year.
Both were treated with the Standard Protocol, which is to say, they were not treated. Think about it. Do you know of any other disease or condition in your lifetime in which the doctor sends you home without prescribing something to help with your symptoms?
Standard Protocol: “Go home, but come back to the ER if your lips turn blue:”
When they became ill and went to the doctor, or ER (I’m not sure which), both my neighbor and the acquaintance mentioned above, were told there was no early treatment for Covid. They were sent home, told to take Tylenol for their discomfort, and to come back to the hospital if their breathing got so difficult that their lips turned blue.
Both dealt with worsening Covid-19 symptoms until they were having difficulty breathing and were very ill. Both were subjected to the toxic protocol of remdesivir and ventilation in the hospital. Both died. It is likely these individuals would have recovered from Covid had they been allowed early treatment, as would many thousands of others.
Dr. Peter McCullough explained in early 2021, that the decision to do nothing led to the worst possible outcomes from Covid-19 – hospitalization and death. He noted that people were often home for 14 days, growing gradually more ill without treatment, until they were hospitalized. McCullough stated, “There’s no immediate lethality to the virus. In fact we’ve got a long window of time to make a diagnosis, organize treatment, and prevent hospitalization and death.” McCullough emphasized:
The different unique aspect of the medical response to SARS-CoV-2 and Covid-19, was for the first time we had an infectious disease where the medical community settled into a group think – and this was supported by the NIH, the CDC, the FDA, the American Medical Association, all the medical societies – to tell doctors, “Don’t touch this virus. Let patients stay home until they get as sick as humanly possible, and then when they can’t breathe anymore, then go to the hospital”…The federal agencies were enormously inept in terms of perceiving what this problem was, incredibly inept. It was just the opposite of what medicine had always been. Medicine had always been early innovation by doctors, emperic treatment…It always started out with early empiricism (knowledge gained through observation and experience) then getting to guidelines and agency statements years later. (emphasis added)
Neglect was often part of the “Covid treatment protocol” in hospitals:
Not only did the federal government financially incentivize a diagnosis of Covid, and interfere with the doctor/patient relationship, but the overall care of Covid patients was often callous. Certainly there were medical personnel who continued to give compassionate care, but there are also many accounts of neglect, and disregard for patients’ treatment preferences and basic needs.
The experience of many Covid patients was that of isolation, lack of food and water, and increasing disorientation. Loved ones often couldn’t visit. Patients couldn’t leave their room. Personnel were hidden behind masks, gloves, and often covered head to toe in protective garb. There was almost no human contact. Medical preferences were ignored and needed medications for chronic conditions were withheld. Some patients were ventilated, not because they were having difficulty breathing, but because the medical staff didn’t want an infected Covid patient openly breathing in the room. Being placed on a ventilator increases the mortality risk for the patient.
Last spring, doctors put patients on ventilators partly to limit contagion at a time when it was less clear how the virus spread, when protective masks and gowns were in short supply. Doctors could have employed other kinds of breathing support devices that don’t require risky sedation, but early reports suggested patients using them could spray dangerous amounts of virus into the air.
-Dr. Theodore Iwashyna, Critical-care physician, December 20, 2020
There are many accounts of the elderly, and the disabled being denied food, even being restrained, and being administered drugs that suppressed them into unconsciousness and death.
A hospital stay is not someone’s best moment, under the most ideal of circumstances. A hospital stay during Covid was the worst of circumstances for patient well-being. We have not yet come to terms with the shocking fact that malpractice and inhumane treatments were rampant during the Covid-19 pandemic. Treatment was sometimes especially egregious if the patient was unvaccinated for Covid-19.
Patients who died under these circumstances may have had Covid-19 listed as the cause of death, but they were actually victims of medical abuse and neglect.
Discarding the Hippocratic Oath during Covid:
“First do no harm” applies as much to using medical knowledge to treat a patient’s symptoms as it applies to not using harmful treatments. It doesn’t mean to blindly follow orders, which is what so many in the medical profession did. For those who say, “But Covid was a new disease and we just didn’t know how to treat it,” comes this answer from Dr. Richard Urso, given during a panel discussion convened by U.S. Senator Ron Johnson in January 2022:
That’s not true, Senator. We knew early on. We had treatment early on from the very first day in March. That’s a fabricated lie [to say we didn’t know how to treat Covid]. It’s scientific fraud to say that. There was treatment for inflammation, there was treatment for blood clotting, there was even treatment that we could try for the virus, there’s treatment for respiratory demise. It was definitely an option…So it’s been a fraud from the beginning. (4:27:40)
But as seen in case after case the doctors, nurses, and scientists who did ask questions, did try to treat patients, and actually did engage in the practice of medicine, have paid an extremely high price.
Disclaimer
Some of the posts we share are controversial and we do not necessarily agree with them in the whole extend. Sometimes we agree with the content or part of it but we do not agree with the narration or language. Nevertheless we find them somehow interesting, valuable and/or informative or we share them, because we strongly believe in freedom of speech, free press and journalism. We strongly encourage you to have a critical approach to all the content, do your own research and analysis to build your own opinion.
We would be glad to have your feedback.

Source: Brownstone Institute Read the original article here: https://brownstone.org/
