
MHRA and Covid Vaccines Surveillance
by Tom Jefferson at Brownstone Institute

Our series on Pfizer’s Comirnaty vaccine was sparked off by a remark from one of our readers.
He is an eye doctor who saw an abnormally high number of cases of Bell’s Palsy during the months of the vaccine’s rollout—perhaps we should say vaccines. Bell’s Palsy is a frightening progressive weakness of facial muscles, usually one-sided. Most cases recover, but some do not. At the time, we asked, “How would you like to go around with half your face hanging down and unable to see properly?”
We have summarised our series of posts on Comirnaty and ask you to refresh your memory before reading further. At the bottom of this post is a series of relevant pieces we have produced since TTE began.
The third of our summary posts wraps up how far we got.
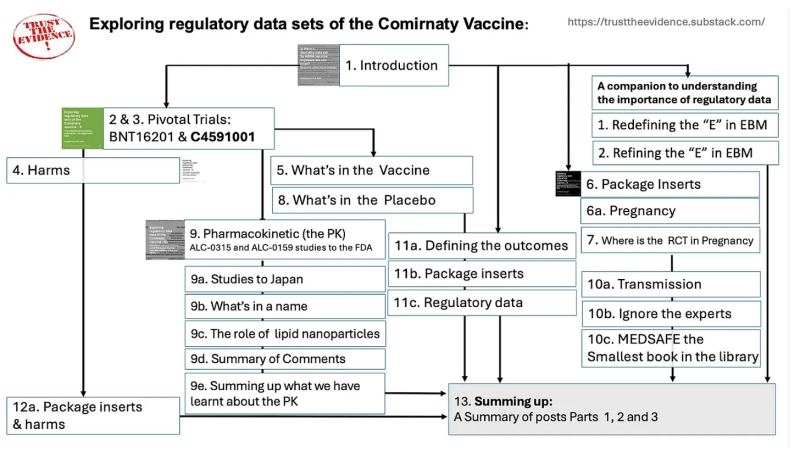
We promised to keep tabs on any major step towards understanding the properties of Comirnaty, having identified some very large gaps in the evidence base.
One of the most contentious parts of the whole saga (apart from the mode of action) is the potential harms of the Covid vaccines. The Oxford AstraZeneca vaccine’s demise is a case in point.
In this post, we reported that in response to a 2022 FOI request on the number of Yellow Card reports for Bell’s Palsy over the previous three years (FOI 21-750), the MHRA responded:
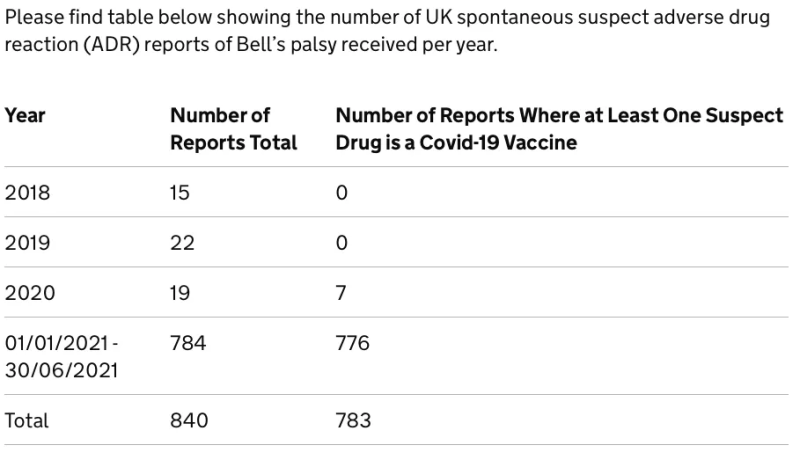
After the table, the responders wrote:
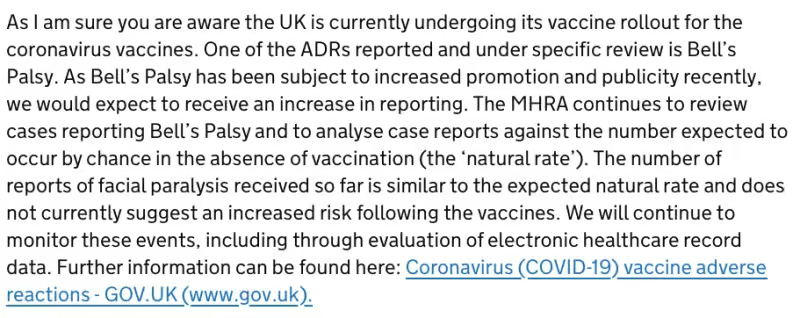
All is well then, thanks to the “evaluation of electronic healthcare record data.” Please remember that.
However, the underreporting rate in the Yellow Card system can be as high as 98%. Anthony Haywood, a member of the public, asked a simple question:
“Dear Medicines and Healthcare Products Regulatory Agency, would you please supply your estimate of the degree of underreporting to your ‘Yellow Card’ scheme, and subsequently your estimate of the actual number of deaths and adverse events, likely to be related to the covid 19 vaccine, at least in the view of the injured party.”
The MHRA’s answer was interesting:
“The MHRA do not hold an estimate of the degree of underreporting to the Yellow Card scheme, nor an estimate of the actual number of deaths and adverse events, likely to be related to the COVID-19 vaccines.”
This is a contradictory statement given that the MHRA reported following up 54% of deaths possibly linked to this or the other Covid vaccines in answering an FOI request.
In the twilight of our neuronal function, we ask: If you do not have an estimate of possible linked vaccine-related deaths, how can you possibly know you are following 54%? Percentage of what we ask?
Of course, they do not have an estimate. They only licensed the stuff, so why on earth would they be interested in its effects?
Nah, you naughty old geezers, they are, they are. One of our subscribers (active lot, are they not?) drew our attention to this newly published preprint:
Oh wow! We thought: this is active surveillance of 30 thousand people who had at least one exposure to one of the Covid vaccines and were prepared to give feedback to MHRA. So we started reading.
First, the authors are employees of MHRA and declare no conflicts and no funding, so it’s intramural work by the “enabler” policing itself for the consequences of its actions. This is straight from the Berlusconi School for studying conflicts: everyone has them, so they balance each other out.
Second, surveillance ended at the end of 2022, so why so long for a pre-print?
Third, YCVM picked up two cases of Bell’s Palsy: one after the first exposure to the AstraZeneca vaccine and the other after a second exposure to Comirnaty. So that’s 2/30,000 over 18 months (0.0067%), which is not quite the same as 783/5 million over six months (0.016%). Standardising annually gives percentages of 0.0045% and 0.031%, respectively.
The difference in these small percentages might seem insignificant, but the MHRA appears to forget—or ignore—what happens when exposures are scaled up to a larger population. Applying to 1 million exposures would result in 45 versus 310 cases of Bell’s Palsy, respectively. Which is it to be?
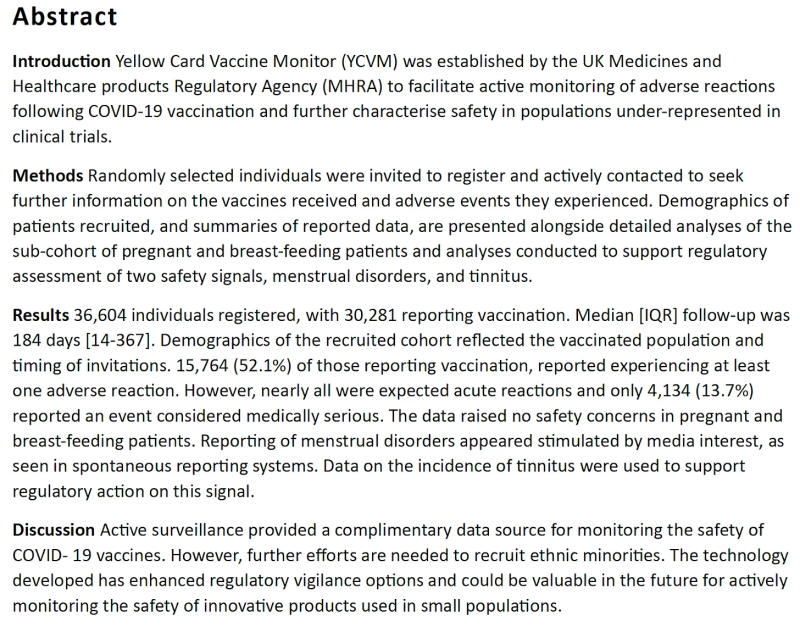
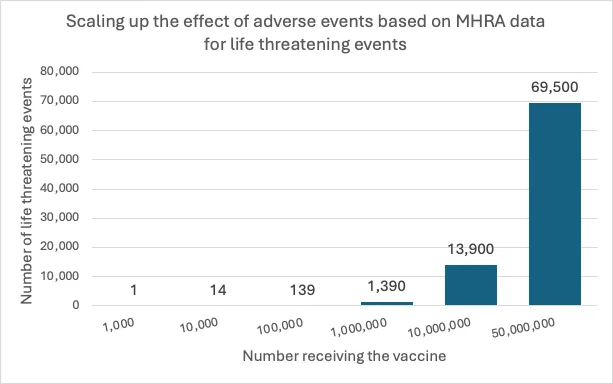
It gets even more interesting as we move further along to Table 5. This table shows the self-reported seriousness of events after any dose or first dose. It took us some time to wade through this table and consider its implications.
We focussed on the life-threatening events and assumed the nonresponders who enrolled in the surveillance did not answer the MHRA because they were busy watching soccer, following Matt Hancock eating lizards, or were just bored. I.e., let’s just assume they were alive and did not fail to respond because they were six feet under.
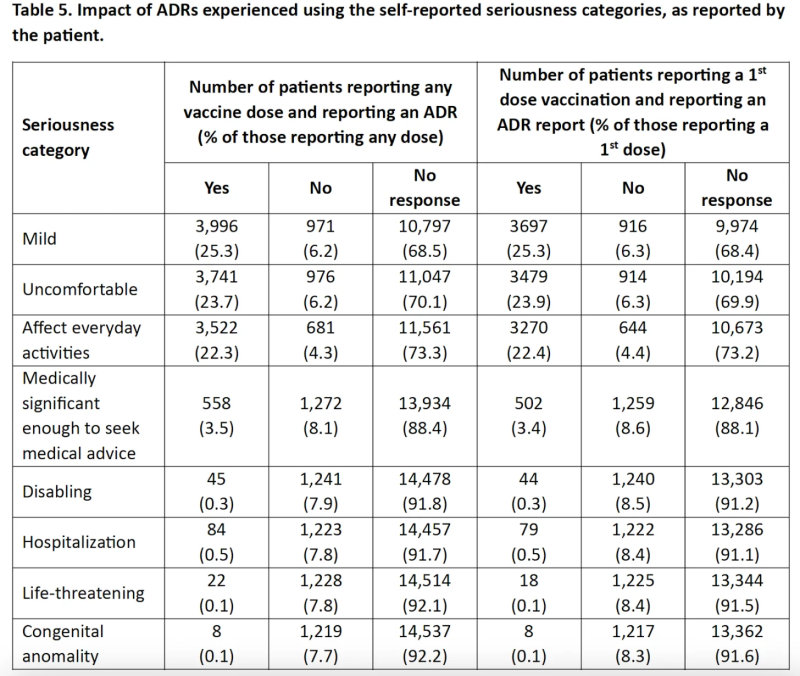
Table 5 reports 22 life-threatening events in 15,764 exposures (0.14%). Again, this might not seem much, but it’s worth considering what happens when you scale this up to the numbers that had the vaccines. We took the figure of 50 million as reported by the BBC to estimate that roughly 69,500 life-threatening events would occur, and in 50 million exposures, we would expect about 350K hospitalisations.
If the MHRA stands by its figures, they might help explain winter pressure and excess mortality.
A further noteworthy statement in the MHRA preprint is,“The YCVM is currently not automatically linked to other sources of health data; therefore, it is impossible to medically confirm self-reported ADRs reported through the YCVM.”
This was particularly important when adverse events of special interest such as GBS and Bell’s palsy were reported. Does that mean MHRA cannot verify the report’s accuracy? If so, why such sweeping conclusions? And what has happened to the 4 billion IT contract the MHRA stipulated early on to facilitate the exchange of information?
We were also perplexed that the COVID-19 Vaccine Surveillance Strategy, published by Public Health England on 11 Jan 2021, stated: “We supplement this form of safety monitoring with other epidemiology studies, including analysis of data on national vaccine usage, anonymised GP-based electronic healthcare records and other healthcare data to proactively monitor safety.”
Which is it to be: we can’t link, or can we?
Finally, a pearl for all our Riddlers: on Table 7, ILI, or Influenza-like illness, is listed as a harm of the AstraZeneca vaccine, but it’s in good company. All the preceding signs and symptoms listed in the table are present in the ILI syndrome, so here’s a further non-infectious cause of ILI. Wham!
This post was written by two old geezers who need the figures checked, please.
Readings
https://trusttheevidence.substack.com/p/is-ebenezer-scrooge-running-uk-pharmacovigilance
https://trusttheevidence.substack.com/p/who-is-running-pharmacovigilance
https://trusttheevidence.substack.com/p/pharmacovigilance-escape-and-evasion
Covid-19 Vaccine Damage Payments Bill Volume 738: debated on Friday 20 October 2023, look at Columns 508-509.
https://trusttheevidence.substack.com/p/the-system-for-reporting-adverse
https://trusttheevidence.substack.com/p/the-system-for-reporting-adverse-122
https://trusttheevidence.substack.com/p/abuse-and-reason
https://trusttheevidence.substack.com/p/why-dame-june-should-stay-on-at-the
https://trusttheevidence.substack.com/p/do-you-think-the-mhra-is-doing-an
https://trusttheevidence.substack.com/p/exploring-regulatory-data-sets-of-ca6
https://trusttheevidence.substack.com/p/exploring-regulatory-data-sets-of-b65
https://trusttheevidence.substack.com/p/exploring-regulatory-data-sets-of-335
https://trusttheevidence.substack.com/p/reflections-on-our-exploration-of
https://trusttheevidence.substack.com/p/kansas-attorney-general-report
https://trusttheevidence.substack.com/p/exploring-regulatory-data-sets-of-3b7
Republished from the authors’ Substack
MHRA and Covid Vaccines Surveillance
by Tom Jefferson at Brownstone Institute – Daily Economics, Policy, Public Health, Society
Disclaimer
Some of the posts we share are controversial and we do not necessarily agree with them in the whole extend. Sometimes we agree with the content or part of it but we do not agree with the narration or language. Nevertheless we find them somehow interesting, valuable and/or informative or we share them, because we strongly believe in freedom of speech, free press and journalism. We strongly encourage you to have a critical approach to all the content, do your own research and analysis to build your own opinion.
We would be glad to have your feedback.

Source: Brownstone Institute Read the original article here: https://brownstone.org/

{kind=link}