

Table of Contents
COVID Transmission/Infection
Falsity #1: Children Can Easily Spread COVID to Adults, Including Their Teachers
Falsity #2: COVID is Easily Spread By Asymptomatic Carriers
Falsity #3: COVID Can Be Easily Spread Just By Someone You Cross on the Street
Falsity #4: COVID Can Be Easily Spread on Surfaces
Falsity #5: You Can Get Re-Infected With COVID
Falsity #6: Social Distancing Is Based On Sound Science
Falsity #7: Mask-Wearing-For-All Is Based On Sound Science
Falsity #8: COVID has started spreading in Wuhan in December of 2019
Falsity #9: COVID is Spreading In An Exponential Manner
COVID Risks/Death Toll
Falsity #10: Returning Children to School is to Gamble With Their Life
Falsity #11: COVID is Very Deadly For the General Population
Falsity #12: COVID is a Death Sentence For The Elderly
Falsity #13: COVID is a Death Sentence For Prisoners
Falsity #14: COVID Has Killed 500,000+ Extra People Around The World This Year
Falsity #15: Cont’d — 2020 Has Been A Very Deadly Year
COVID Policies/Treatments
Falsity #16: We Need More Ventilators
Falsity #17: Lockdowns Have Saved Millions of Lives
Falsity #18: Sweden Was Reckless in Its COVID Approach And Failed
Falsity #19: Every Life Counts, And Lockdowns Don’t Have Health Consequences
Falsity #20: Those Who Question the Corona-Panic Narrative Are Conspiracy Theorists
Falsity #21: The US is Facing a Dangerous 2nd Wave
Falsity #22: We’re Very Far From Herd Immunity, And Reopening Too Early Is Deadly
When Will The Corona Madness End?
On March 24th, right around the time I urgently came back to Quebec with the family over the fears that the entire country of Canada was about to lockdown to stop the spread of a terribly deadly virus, Dr. Didier Raoult — considered the #1 expert worldwide in Communicable Diseases — called the COVID crisis a “collective hallucinated drama” [translation mine, from French].
That same week, John Ioannidis — professor of medicine and epidemiology at Stanford, one of the most influential US-based scientists alive, and described as “the scourge of sloppy science” by the BMJ, said that the COVID crisis might end up being a “once-in-a-century evidence fiasco”.
Another “COVID skeptic” — Dr. Sucharit Bhakdi, medical doctor and specialist in microbiology, and one of the most cited research scientists in German history — said that “all these [COVID-related] measures are leading to self-destruction and collective suicide based on nothing but a spook.”
These statements left me speechless. Were all these prestigious scientists right, or completely out of their darn minds? Was our reaction to this virus completely exaggerated? Were we in the middle of a mass hysteria event?
In the first article I published on the topic on April 1st, I chose to be extremely prudent considering the climate at the time… and simply said that there were a lot of “inconvenient facts” that had been ignored in the entire COVID narrative we had been hearing for weeks.
Then I dove even deeper, spent way too much time looking at the crisis from all angles to make sure I wasn’t the one losing my mind, and at the end of May/early June I published a new 3-part article series.
That’s where I made the case that the world has been turned upside down over a virus that’s orders of magnitude less dangerous/deadly/serious/threatening than the Imperial College London had originally predicted (reminder: they said 2.2M Americans would die if we did nothing, and 1.1-1.2M if we did everything perfectly…).
Months later, the scientific data is confirming what Ioannidis and others have been suspecting for months: COVID was a pandemic similar to a harsh flu season, and the global reaction to this virus was rooted in sheer panic, not in sound and rational science-based policies.
This article will be very different from my previous ones. I don’t have hundreds of hours to put into a 30,000 word article, so I’ll make my points short, and will simply present a list of falsities that have been said about COVID, and give you a few links to read further on each one of them, should you want to go deeper.
Again — if I didn’t make that clear in my previous posts — if you want to comment below, be warned that I will tolerate zero ad hominem attacks, useless politics, and other nonsense. Stick to commenting/discussing/debating the facts that are presented and you’ll automatically become more rational than the vast majority of journalists, scientists, doctors and laypeople I’ve seen comment on COVID since the beginning of this madness.
COVID Transmission/Infection
Falsity #1: Children Can Easily Spread COVID to Adults, Including Their Teachers
“Scientists now know young children don’t transmit the virus.”
— Dr. Daniel Koch, Switzerland Health Ministry’s infectious diseases chief
Nope. We’ve known for months that children extremely rarely transmit COVID, possibly because their virus load is smaller compared to adults.
In fact, some scientists recently shared that they could not find a single case in the world where a child infected a teacher.
- In the French Alps, a 9-year-old child was in contact with 172 people, and transmitted COVID to only one of them (source)
- In the Italian town of Vo, which was under a complete lockdown very early and where almost all residents were tested, not one child under 10 (out of 234) tested positive for the virus (source)
- Dr. Ebere Okereke, a consultant in global public health for Public Health England, has recently claimed — based on a recent review of the evidence done by the Royal College of Paediatrics (RCP) — that “children do not appear to transmit coronavirus”. “So no risk of children passing it on to their teachers – or their parents or their grandparents” (source)
- There are many other sources on that topic in my latest article here.
Falsity #2: COVID is Easily Spread By Asymptomatic Carriers
“The problem is the political pushback, presumably motivated by fear, because [Dr. Van Kerkhove] was correct in her facts. […] The fact is that a huge percentage — 50% or more — of those who are infected are asymptomatic.
The other fact that she said is true, it’s not common — in fact, it’s rare to get an infection transmitted by an asymptomatic person. […] She was quoting the studies, but what we should be saying is from the studies.”
— Dr. Scott Atlas, senior fellow at Stanford University’s Hoover Institution and former chief of neuroradiology at Stanford University Medical Center
On June 8th, Dr. Maria Van Kerkhove, head of the WHO’s emerging diseases and zoonosis unit, said that asymptomatic spread of COVID is “very rare”. Then, two days later, the WHO slapped her wrist and had her “walk back” on her statements.
But the reality is that Dr. Kerkhove was completely right — the best scientific data we currently have from countries who have done extremely detailed contact tracing does show that transmission from asymptomatic carriers is very rare!
In plain English? The little science we do have supports the idea that people who do not currently display symptoms of COVID, very rarely transmit COVID. If this is true, it begs the question why we are moving forward with mandating masks and continuing the social distancing game?
As it is the case during flu season, people who display any kind of flu-like symptom should stay home, period.
Falsity #3: COVID Can Be Easily Spread Just By Someone You Cross on the Street
“There is no significant risk of catching the disease when you go shopping. Severe outbreaks of the infection were always a result of people being closer together over a longer period of time.” [emphasis mine]
— Professor Hendrik Streeck, HIV researcher, epidemiologist, clinical trialist and professor for virology and the director of the Institute of virology and HIV Research at the University Bonn
The data we have shows that COVID does not spread easily in people you are in contact with for just a few seconds, or even a few minutes. In reality, the main vectors of transmission are prolonged contact inside near a COVID carrier, and nosocomial (hospital-acquired).
This shows that wearing a mask outside is downright silly, and that wearing a mask outside while jogging is even more insane.
- Study: Out of 318 COVID clusters across China with 3 or more infections, not one occurred outside.
- From early March (was valid then, and still holds true to this day): “‘Casual contact’ isn’t cause for concern at the moment, as most recorded cases of community transfers are from people who have been in close contact with the infected person for prolonged periods of time. The chances of someone contracting the virus from a casual contact are ‘fairly low’” (source).
- New England Journal of Medicine, Universal Masking in Hospitals in the Covid-19 Era: “Public health authorities define a significant exposure to Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes)”.
- Masks Likely Do Not Inhibit Viral Spread by Dr. Joseph Mercola
Falsity #4: COVID Can Be Easily Spread on Surfaces
“We know [COVID] is not a smear infection that is transmitted by touching objects, but that close dancing and exuberant celebrations have led to infections.”
— Professor Hendrik Streeck, HIV researcher, epidemiologist, clinical trialist and professor for virology and the director of the Institute of virology and HIV Research at the University Bonn
Nope. The CDC has been saying for months that transmission on surfaces is unlikely. As soon as early April, German virologist Hendrik Streeck found that COVID cannot be easily transmitted on surfaces, after studying grocery stores, hairdressers and other public places.
Falsity #5: You Can Get Re-Infected With COVID (Just After You’ve Had It)
“Patients in South Korea who re-tested positive had very little to no ability to spread the virus.”
— Korea Centers for Disease Control and Prevention (source)
Many hypothesized that the reason some people previously tested positive for COVID, then tested negative (showing they didn’t have the virus anymore), only to then re-test positive is that the tests were not precise enough, and produced a huge amount of false-positive results. I talked about this issue extensively back on April 1st.
Since late May, Korean researchers have confirmed that you cannot get reinfected with COVID, and that these seemingly positive tests people get after being infected and recovering are just false-positives.
“As a result of these findings, published online Tuesday, the South Korean CDC no longer recommends that people in this situation be isolated.”
I personally know someone who works in one of the nursing homes in Montreal where the COVID death toll has been among the worst, and he has confirmed that as of few weeks ago, staff members who test positive and then follow a 14-day quarantine period (South Africa recently reduced this period to 10 days after new evidence came in) can go back to work without additional testing. (Too many of them tested positive again, but even health officials now recognize that the tests are too often bogus.)
All that being said, it’s true that immunity to COVID, just like it is the case with other coronaviruses, might last for just a few years. It’s known that most people get reinfected with cold-inducing coronaviruses around every 5 years.
- Good News, Reinfection Unlikely by Dr. John Campbell
Falsity #6: Social Distancing Is Based On Sound Science
“Handwashing and encouragement are what we need, not formalised rules. This means trying to keep a distance from each other where possible and avoiding spending time indoors in crowded places. Much of the evidence informing policy in this outbreak is poor quality; let us hope that evidence-informed decision-making will at some point resume.” [emphasis mine]
— Carl Heneghan (director) and Tom Jefferson (honorary research fellow), Centre for Evidence-Based Medicine, University of Oxford
Stay two meters/6 feet apart? Why has the WHO been recommending 1 meter from the very beginning?
The idea of social distancing is thought to have originated in a 14 year old’s science fair project. The distance that has been used in different countries has been “conjured out of nowhere”, certain countries like the US and Canada essentially doubling WHO’s 1 meter rule to “be on the safe side”.
Social distancing has never been scientifically proven as a valid tool to slow down or stop the spread of a respiratory virus. Its efficacy is unknown.
Given all this, my humble opinion is that we should at least stick with the 1 meter rule which will make it possible to save many struggling businesses like restaurants and bars that are currently going bankrupt.
- Jefferson and Heneghan from the Oxford Centre for Evidence-Based Medicine: “There is no scientific evidence to support the disastrous two-metre rule”
Falsity #7: Mask-Wearing-For-All Is Based On Sound Science
“It is also clear that masks serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers’ perceived sense of safety, well-being, and trust in their hospitals. […] Expanded masking protocols’ greatest contribution may be to reduce the transmission of anxiety, over and above whatever role they may play in reducing transmission of Covid-19.” [emphasis mine]
— Recent study by researchers from the Department of Population Medicine, Harvard Medical School and Harvard Pilgrim Health Care Institute (M.K.), Brigham and Women’s Hospital (M.K., C.A.M., J.S., M.P.), Harvard Medical School (M.K., C.A.M., E.S.S.), and the Infection Control Unit and Division of Infectious Diseases, Massachusetts General Hospital (E.S.S.) — all in Boston.
The science behind the efficacy of face masks in entire populations to slow down the spread of COVID (or any respiratory infection) is flimsy at best.
Denis Rancourt, PhD, explains:
“There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.” [emphasis mine]
The Occupational Safety and Health Administration (OSHA) website confirms that both cloth face masks and surgical masks “will not protect the wearer against airborne transmissible infectious agents due to loose fit and lack of seal or inadequate filtration.” (source)
- Dr. Brosseau — national expert on respiratory protection and infectious diseases and professor (retired), University of Illinois at Chicago: Masks-for-all for COVID-19 not based on sound data
- Impact of non-pharmaceutical interventions against COVID-19 in Europe: a quasi-experimental study: “requiring the wearing of facemasks or coverings in public was not associated with any independent additional impact.”
- New England Journal of Medicine, Universal Masking in Hospitals in the Covid-19 Era: “It is also clear that masks serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers’ perceived sense of safety, well-being, and trust in their hospitals. […] Expanded masking protocols’ greatest contribution may be to reduce the transmission of anxiety, over and above whatever role they may play in reducing transmission of Covid-19.” In other words, the protection masks offer is more psychological than physiological…
- June 2020: Do facemasks protect against COVID‐19? “During [previous] pandemics […], many people in Asia and elsewhere walked around wearing surgical or homemade cotton masks to protect themselves. One danger of doing this is the illusion of protection. […] A pre‐symptomatic or mildly infected person wearing a facemask for hours without changing it and without washing hands every time they touched the mask could paradoxically increase the risk of infecting others.” [emphasis mine]
Falsity #8: COVID has started spreading in Wuhan in December of 2019
“As I’ve been saying, with a rapid and completely novel virus, and daily flights from Wuhan to LA, SF and Europe, the idea that this virus wasn’t everywhere back in November or even earlier is now impossible to defend.”
— Joel Hay, PhD, Professor of Pharmaceutical and Health Economics, USC School of Pharmacy
In the last several months there’s been several indications that this is completely implausible and untrue. The virus was around way sooner than we previously expected, and has likely not originated from a market in Wuhan.
This explains why lockdowns and most interventions have been highly ineffective in slowing down infections. The virus had already spread widely, and can hardly be “controlled”.
- The first confirmed COVID case in the US was not in Washington State on February 29th as previously thought, but on February 6th in California (source)
- COVID has been identified in sewer samples in Barcelona, dating back from March of 2019 — this still needs to be confirmed but would change the entire timeline, again (source)
- The first case in France was identified on November 16th, 2019 (source)
- The first case in Quebec, Canada is suspected to be in December of 2019 (source)
- COVID was already present in Italy in mid-December, as reported by Italian officials (source)
- Genetic studies indicate that the virus was spreading all around the world in late 2019 (source)
- SARS-CoV-2 in human sewage in Santa Catalina, Brazil, November 2019 (source)
Falsity #9: COVID is Spreading In An Exponential Manner
“We see now, by just looking at the data, that from the very first confirmed case, the rate of growth of COVID-19 is not constant. It’s growth is never exponential.” [emphasis mine]
— Michael Levitt, winner of the 2013 Nobel in Chemistry
This meme has been constantly repeated in the media, and was included in the original ICL paper that made the world panic.
The truth is that starting from early February but probably sooner, it was already clear that the spread of the virus did NOT follow an exponential curve.
- 2013 Nobel winner Michael Levitt: COVID19 Never Grows Exponentially
- Mathematician Andrew Mather: Covid-19: Debunking the Exponential-Lockdown lies so beloved by Gates, Johnson, Ferguson, Hanington
COVID Risks/Death Toll
Falsity #10: Returning Children to School is to Gamble With Their Life
“The risk of death in children is about one in five and a half million and they’re rather more likely to die in road accidents or even from lightning strikes than from the virus.”
— Robert Dingwall, professor of sociology at Nottingham Trent University whose focus is on the interdisciplinary study of law, medicine, science and technology, and member of the UK government’s Emerging Respiratory Virus Threats Advisory Group (NERVTAG)
Completely wrong. We now have months of data which clearly shows that children are in fact less likely to die from COVID than the flu.
There have been and will always be some exceptions, in children who are immunocompromised, for example. These children are at risk from dying from many transmissible diseases, including the flu. That being said, the idea that COVID was responsible for “rare cases of a Kawasaki-like disease” has been recognized weeks ago as a non-issue.
Millions of kids have returned to school since May in many European countries, without a significant increase in both COVID cases and COVID-related deaths.
- Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units: “Thus, up to this time of the pandemic in North America, children continue to face a far greater risk of critical illness from influenza than from COVID-19”
- Dr. Malcolm Kendrick, author of Doctoring Data: How to Sort Out Medical Advice from Medical Nonsense: “How many people aged 15 or under have died of Covid-19? Four. The chance of dying from a lightning strike is one in 700,000. The chance of dying of Covid-19 in that age group is one in 3.5million. And we locked them all down.” (source)
- Dr. Andrew Bostom, associate professor of family medicine (research) at the Warren Alpert Medical School of Brown University: “The relatively benign nature of COVID-19 in children, compared to seasonal influenza, should further give us pause. For example, using mortality data available through May 8, 2020, U.S. children 0-14 years old were ~7 times more likely to die from influenza this year, despite vaccination programs, than from COVID-19.”
Falsity #11: COVID is Very Deadly For the General Population
“This is nothing more than a flu epidemic if you care to look at the numbers and the data, but people who are in a state of anxiety are blind.”
— Yoram Lass, former Director-General of Israel’s Health Ministry
Scary images coming from Italy, and then New York, made the world panic, but that panic is unsubstantiated. The reality is that COVID has a lethality similar to a harsh flu season — with an Infection Fatality Rate (IFR) of anywhere between 0.1-0.5%.
A telling example is that more people under 45 years old in the UK have died in traffic accidents than from COVID this year.
- Find a list of dozens of serological studies and analyses which support the idea that COVID is as lethal or even less lethal than the flu: https://theemfguy.com/covid-part2/#t41
- Extensive list of PCR and serological studies around the world showing an average IFR of 0.38% (thanks to SPR).
- Many international experts such as Prof. Sunetra Gupta from Oxford still predict that the final IFR of COVID will be closer to 0.1%, similar to the seasonal flu.
Falsity #12: COVID is a Death Sentence For The Elderly
“There’s some sort of mob mentality here operating that they just insist that this has to be the end of the world, and it has to be that the sky is falling. It’s attacking studies with data based on speculation and science fiction. […] But dismissing real data in favor of mathematical speculation is mind-boggling.”
— John Ioannidis, professor of medicine, of epidemiology and population health, of biomedical data science, and of statistics at Stanford University and co-director of Stanford’s Meta-Research Innovation Center. Among the top 100 most cited research scientists worldwide
There’s no denying that COVID is very deadly in the elderly, especially in people who are 80+ and who have multiple chronic conditions.
But it still isn’t clear if COVID is any more deadly than other coronaviruses which are already known to be very dangerous in the elderly, or even more dangerous than the flu. In a recent interview, 2013 Nobel prize winner Michael Levitt said that the age profile of those who died from COVID across Europe is virtually identical to people who normally die from the flu.
The difference between these two respiratory viruses is that COVID-19 is more recent, less understood, and that fewer treatment options are available. The future will tell, but we can already say that COVID is simply nothing like the Spanish flu — a completely irresponsible comparison that the World Health Organization (WHO) kept making throughout this crisis.
- Many analyses have shown that the risk of dying from COVID is similar in the elderly as the overall risk you face from old age. (see here, just one example) If this is true, the vast majority of our elders — and the rest of society — can simply go back to normal while we take extra care to protect the nursing homes, where the real COVID crisis has been.
- Very recently, a study done by the UK government found out that more than 80% of all care home residents who tested positive for COVID were asymptomatic — further indications that the final lethality of COVID will likely be multiple times lower than we previously thought.
- How much ‘normal’ risk does Covid represent? by David Spiegelhalter, Winton Centre for Risk and Evidence Communication
Falsity #13: COVID is a Death Sentence For Prisoners
“And take prisoners: 2.3 million American prisoners … and only 35 deaths? Here we have forced social mixing, and less deaths than the rest of the country. C’mon. How do they explain that?” [Note: that’s an older quote, but the death rate is still so low among prisoners months later that it still holds true. 681 as of July 14th.]
— Joel Hay, PhD, Professor of Pharmaceutical and Health Economics, USC School of Pharmacy
The freakout about prisoners is one of the most bizarre parts of this COVID madness. About 8,000 prisoners will be released from the Newson prison in California by the end of August over fears of COVID outbreaks.
The problem? An April study performed in 4 State prisons revealed that 96% of prisoners who were COVID-positive were asymptomatic. As of July 8th, the death rate in prisons was 39 per 100,000 prisoners — which equals an IFR (infection fatality rate) of… 0.039% — around 3 times less than the flu. The question is: Do we normally release prisoners earlier because of the seasonal flu?
Falsity #14: COVID Has Killed 600,000+ Extra People Around The World This Year
“A lot of the people that died from COVID would have died anyway, sadly, in that period.”
— Professor Karol Sikora, Founding Dean and Professor of Medicine at the University of Buckingham Medical School and an ex-director of the WHO Cancer Programme
Sensationalistic coverage of the death toll has made most people believe that everyone who (allegedly) died from COVID has died prematurely, and would have otherwise survived and thrived for years.
The reality is that many experts agree that a very large fraction of COVID victims would have not survived the year anyway, and would have died from something else. I’m not sharing this without sadness, since this reflects the tragic reality that we have millions of elders worldwide who are extremely sick at the end of life (often in nursing homes), and at risk of dying from respiratory infections that are essentially mild for the rest of the population.
- Professor Sir David Spiegelhalter, statistician at Cambridge University: “Many people who die of COVID would have died anyway within a short period.” (source)
- Professor Neil Ferguson from the Imperial College London, AKA “Mr. Lockdown” himself: “The proportion of COVID victims who would have died anyway could be ‘as many as half or two-thirds’.” (source)
- Professor Klaus Püschel, forensic doctor at the University Medical Center Hamburg-Eppendorf (UKE): “All of his autopsies who died of COVID had previous illnesses and would not have survived this year anyway.” (source)
Falsity #15: Cont’d — 2020 Has Been A Very Deadly Year
“The excess deaths from COVID [in Europe] are actually 15% more than the flu season of 2017-2018.”
— Michael Levitt, winner of the 2013 Nobel in Chemistry
This will leave many people speechless, but it’s the truth. All around the world, the COVID pandemic has not led to a very large increase in overall mortality that’s above what has been seen in previous flu seasons.
The latest data (July 5th 2020) from Europe, analyzed by Ivor Cummins, clearly shows that excess mortality has barely increased compared to the 2017-2018 flu season.
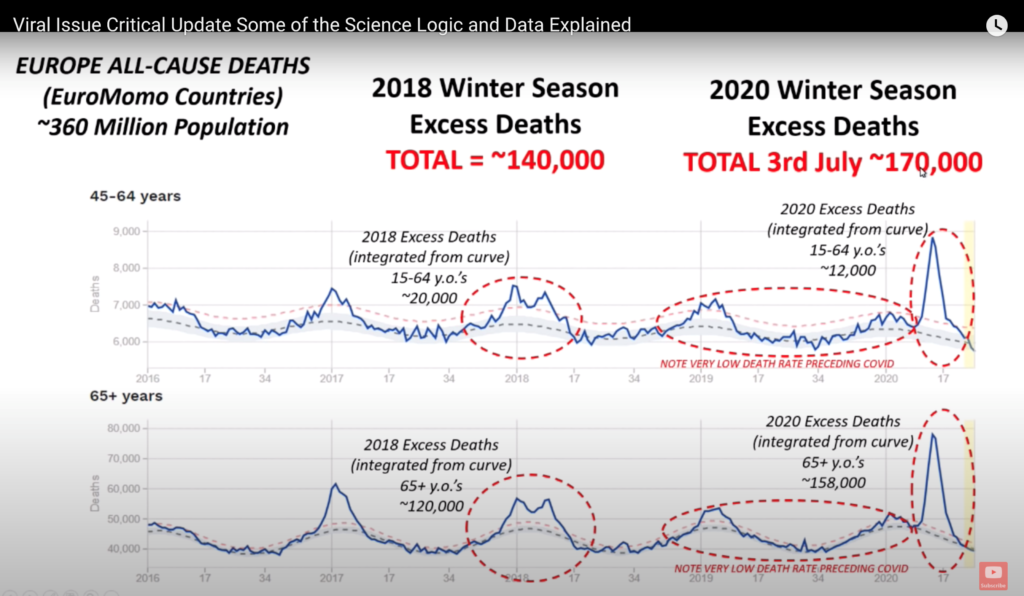
In other countries, overall mortality has not increased compared to previous years (see sources below), begging the question… where is the deadly pandemic everyone has been talking about for months?
- USA: USC Professor of Health and Pharmaceutical Economics Joel Hay, PhD, maintains that overall mortality has not increased so far, and that while we did see a huge initial spike in mortality in the beginning, overall mortality is now well under the yearly average. See this tracker created by researchers at the National Cancer Institute Division of Cancer and Epidemiology and Genetics.
- Sweden: Overall mortality has not been worse than previous years, which essentially means that COVID cannot even be seen in their statistics. Their new COVID deaths and hospitalizations are near zero (as of early July), and they already seem to have herd immunity.
- UK: Overall mortality is slightly worse than the 2017-2018 flu season, but less than during the 1999-2000 flu season.
- Norway: Overall mortality during this COVID year is below average.
COVID Policies/Treatments
Falsity #16: We Need More Ventilators
“More ventilators!’ cried the journalists on Twitter. ‘Yes, more ventilators!’ replied the politicians. ‘Where are the ventilators?’ demanded the journalists, now screaming on television. ‘Yes, even more!’ replied the government, somewhat nonsensically.
I am a critical care physician, specialising in the use of such machines. I’m flattered by all the attention our tools are receiving. But I fear the current clamour reminds me of nothing so much as the panic buyers of toilet-paper stampeding over each other in early March.” [emphasis mine]
— Dr. Matt Strauss, former medical director of the critical care unit at Guelph General Hospital, Canada, and assistant professor of medicine at Queen’s University
This might have seemed true at first, but it’s rapidly been increasingly clear that ventilators are the wrong medical intervention against COVID in a lot of cases.
Data from late April in New York City confirmed that an extremely high number of patients (97.2% over 65 years of age) who were put on ventilators died. Normally, you would expect around 40 to 50% of patients with severe respiratory distress to die while on ventilators.
Ventilators are still a useful tool in certain situations, but clearly have not been a panacea in treating COVID patients, and might have done more harm than good in many situations.
- Dr. Matt Strauss: Ventilators aren’t a panacea for a pandemic like coronavirus
Falsity #17: Lockdowns Have Saved Millions of Lives
“Scientists are getting away scot-free for causing billions of dollars’ worth of damage and this is something that cannot be allowed to happen. It’s not just the World Health Organisation. Ferguson wanted Sweden to lockdown, got Britain to lockdown, and when the numbers become normal, exactly what you would expect without lockdown.
He then says, ah it’s because of lockdown. This is terrible science. This is science which should go on trial. Scientists cannot cause damage like this and refuse to listen.” [emphasis mine]
— Michael Levitt, winner of the 2013 Nobel in Chemistry
This is the flawed belief that explains why most people are still on the COVID apocalypse bandwagon.
The math seems simple: COVID was deadly, and millions were predicted to die. We locked down. We saved millions of lives.
But the reality is: COVID was like a bad flu, and the predictions were wildly exaggerated. The lockdown came in way too late since COVID was already circulating around the globe back in December 2019, and in most countries COVID cases peaked before the lockdown. (I explained this in length in part #3 of my last article).

Image source: The Flawed COVID-19 Model That Locked Down Canada, iedm.org
In reality, there’s simply no correlation that can be established between lockdowns and a reduction in COVID cases, or COVID deaths. Quite the opposite: Oxford’s data on 160 countries showed that the more strict lockdowns were, the more COVID infections — possibly because most COVID infections are due to close proximity in enclosed spaces.
A recent study published in the Lancet which included data from 50 countries showed that lockdowns did not led to a significant reduction in COVID deaths, or the number of critically ill patients.
- Military scientist Prof. Isaac Ben-Israel has also demonstrated that “simple statistics show the spread of the coronavirus declines to almost zero after 70 days — no matter where it strikes, and no matter what measures governments impose to try to thwart it” (source)
- Ivor Cummins: Ep80 The Latest DATA and EVIDENCE – Have our Lock-downs been Effective?
Falsity #18: Sweden Was Reckless in Its COVID Approach And Failed
“We have really, really failed as a group. There have been smart people in Sweden, and that’s about it.
[…] Sweden is the only country that has done the right thing by heading for what they consider to be herd immunity. It occurs at 15%, not at 80%, another error that the epidemiologists made. Sweden is going to end up with about 600 deaths per million.” [emphasis mine]
— Michael Levitt, winner of the 2013 Nobel in Chemistry
People who still cling to the idea that lockdowns saved millions of lives point the finger at Sweden and argue that their approach has “failed”, considering they have a higher mortality compared to their neighbouring countries.
In reality, Sweden has now reached herd immunity, and their ICUs are now essentially free of COVID patients. Their overall mortality has not increased (also see here) compared to previous years. And they stand in the middle of the pack internationally when it comes to COVID deaths per million capita.
Where Sweden — and virtually all other countries — did fail in a major way is when it comes to protecting nursing homes early. This was not done properly, and explains why 50% of their COVID deaths were in nursing homes. This number has been similar in Canada, the US and 24 other countries.
- Ivor Cummins: Viral Issue Critical Update Some of the Science Logic and Data Explained (in depth review of Swedish data, no increase in excess deaths)
- Daniel Hannan, late April: If Sweden succeeds, lockdowns will all have been for nothing
- Joel Hay, PhD, expert in public health policy: “It is now absolutely clear that Sweden did it correctly by NOT locking down, and the rest of the world, particularly the US, created enormous additional disease and suffering with the destructive lockdowns.” (source)
- Michael Levitt: “Sweden is the only country that has done the right thing by heading for what they consider to be herd immunity. It occurs at 15%, not at 80%, another error that the epidemiologists made. Sweden is going to end up with about 600 deaths per million.”
Falsity #19: Every Life Counts, And Lockdowns Don’t Have Health Consequences
“I’m still projecting more than 100 lockdown deaths for every C19 death avoided through lockdowns! Anyone could have foreseen that the economic and health consequences of the lockdowns were going to be severe and fatal.”
— Joel Hay, PhD, Professor of Pharmaceutical and Health Economics, USC School of Pharmacy
Trying to prevent everyone from dying from everything has never been, and will never be a viable strategy. But COVID is the exception.
Many pro-lockdown people afraid of COVID tried to argue that those who were against end of lockdowns put money before lives.
In the end, the debate for me has always been lives VS lives — the health cost of the economic devastation and the side effects of the lockdown, versus how many lives the lockdown itself will save by slowing down the spread of COVID and preventing hospitals from being overwhelmed.
Dr. David Katz, former director of the Yale-Griffin Prevention Research Center, is one of the few experts who’s been openly talking about this devastatingly ignored issue:
“There is more than one way for this pandemic contagion to hurt people. It can hurt them directly via infection, and it can hurt them indirectly via our responses to the contagion. And both are bad, preventing both is good, and we should be gathering more data […] to navigate between those two perils.”
Many health experts already predict that the death toll from COVID-related lockdowns will be much, much worse than from COVID itself (see sources below).
- See section 5.3 of my latest article for a long list of lockdown-related deadly consequences
- Perspectives on the Pandemic | Dr. David L. Katz – by Journeyman Pictures
- “According to a preprint in the Lancet, more than one million children under five and 60,000 more mothers could die in the next six months alone as a result of disruptions to health services caused by the pandemic in low- and middle-income countries.” (source)
- Mathematical models (that I sure hope are wrong) predict that hundreds of thousands will die from tuberculosis in the next years because of the COVID-related lockdowns which prevented proper screening and treatments. (source)
- Professor Karol Sikora, former advisor to the WHO on cancer care, estimates that way more people will die from a lack of cancer screening in the UK than there have been COVID victims (source).
- Nobel-winning Michael Levitt: “We should never have listened to the epidemiologists. […] They have caused hundreds of billions of dollars’ worth of suffering and damage, mainly on the younger generation. […] It’s going to make 9/11 look like a baby story.” (source)
- We already know that 5,000 already died in the UK from heart attacks because of a lack of proper urgent care (source)
Falsity #20: Those Who Question the Corona-Panic Narrative Are Conspiracy Theorists
“I was just explaining what [science] we had. […] They don’t tell you. They just say it violates our community standards. There’s no explanation for what those standards are or what standards it violated.”
— Knut M. Wittkowski, former head of biostatistics, epidemiology, and research design at Rockefeller University, who got entirely banned from YouTube for offering a scientific analysis of the COVID data that goes against the current narrative
The world has been turned upside down, and even Dr. Sucharit Bhakdi, one of the most cited research scientists in German history, has been called a “conspiracy theorist”.
John Ioannidis (top 100 scientists in the world) has been attacked for his calm, rigorous, science-based analysis of the COVID data. His response was: “There’s some sort of mob mentality here operating that they just insist that this has to be the end of the world, and it has to be that the sky is falling. It’s attacking studies with data based on speculation and science fiction. […] But dismissing real data in favor of mathematical speculation is mind-boggling.”
2013 Nobel in Chemistry winner Michael Levitt has revealed in a recent Lindau Nobel Laureate meeting that he has received nothing but “abuse” from his fellow scientists since he started analyzing the COVID data and quickly predicted that the initial projections made by the Imperial College London were off by a factor of at least 10-fold.
The COVID story that has been presented in the media has been one-sided, and these scientists whose research came to different conclusions than what was popular at the time were simply not invited on mainstream media shows to share their opinions.
Being skeptical towards the COVID narrative doesn’t make one a conspiracy theorist, a pro-Trumper, or an insane person. It’s probably the opposite.
Falsity #21: The US is Facing a Dangerous 2nd Wave
“OF COURSE THERE ARE RECORD CASES! WE’RE TESTING LIKE MAD! It would be a shock if we didn’t see a surge in new “cases” with all this testing!
Pardon my screaming, but we have gone, as the phrase has it, stark raving mad. I am beside myself with frustration trying to explain this to people who are so panicked they can’t listen to reason.” [emphasis mine]
— William M. Briggs, PhD from Cornell University in statistics, writer, philosopher and scientist
I had been warning my readers in Part 1 of my last article series that the media would start reporting on “scary COVID outbreaks” when we start ramping up our testing capabilities. That’s exactly what happened.
Since COVID-related hospitalizations and COVID-related deaths are constantly dropping, it seems that COVID alarmists are re-focusing their attention on COVID cases, and how they have been increasing.
In reality, the COVID-positive test rate (what fraction of all COVID tests are positive) has not increased by much — going against the idea that COVID is spreading exponentially once again.
Here’s how the number of daily tests in the US has evolved over time:
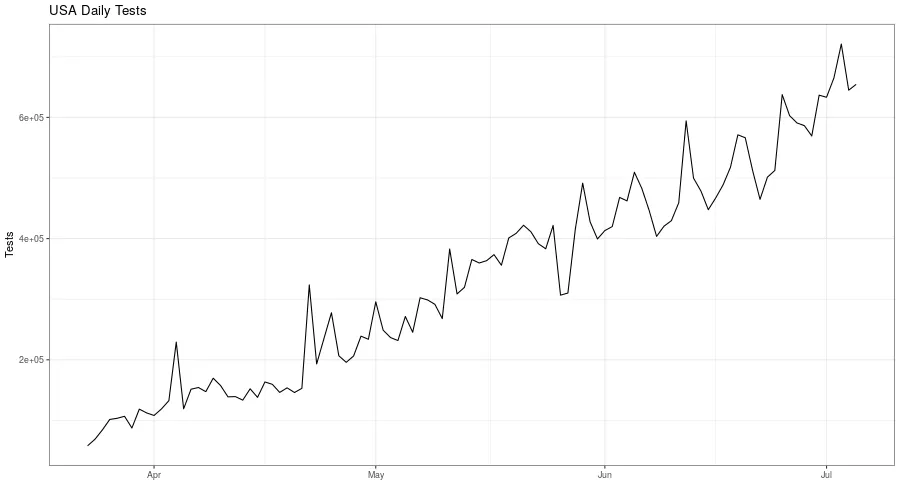
Image source: Statistician William M. Briggs
And here are tests over time, compared to the COVID-positive test rate:
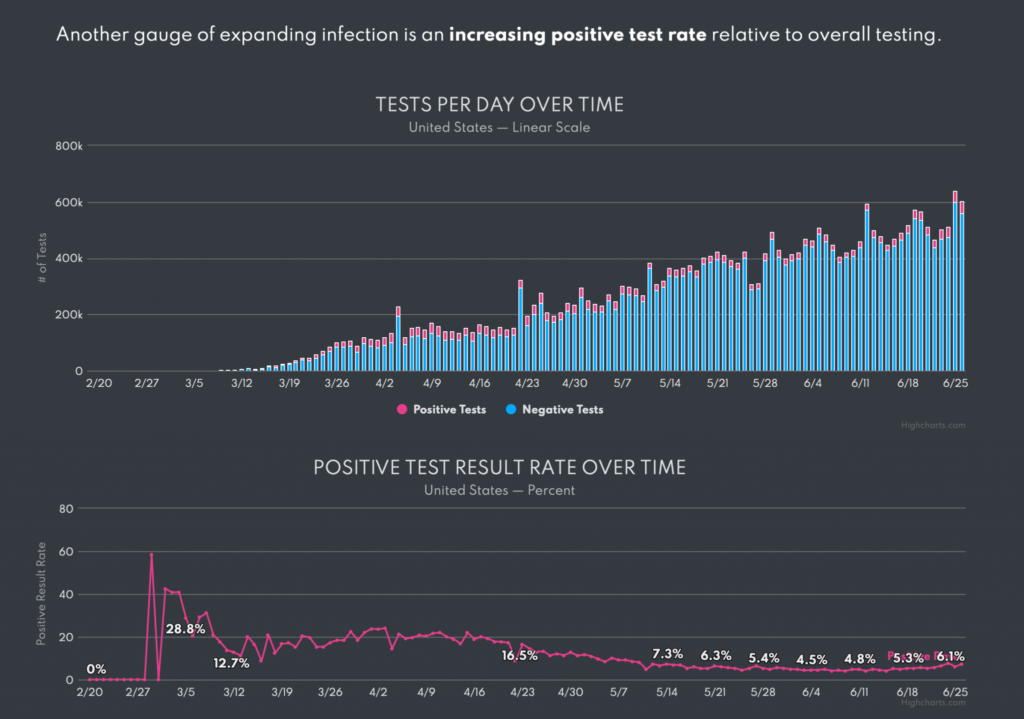
Image source: Lockdown Skeptics
In the meantime, the COVID-related deaths are still going down — that’s the real figure we need to look at:

Image source: Statistician William M. Briggs (CDC data, ending July 20th)
- Statistician William H. Briggs: Coronavirus Update XXI: Calm Down! Record Testing Is Why There Are Record “Cases”
- Also see his next article Coronavirus Update XXIII: Yes, More Testing Leads to More ‘New’ ‘Cases’
- After a week of apocalyptic media coverage about the 70,000 new cases in Florida, reporter Alex Berenson found out that the ICU admissions had increased by just 130 — in a State with a population of more than 20M people…
- Joel Hay, PhD, has pulled out the overall mortality data from Texas, Florida and California, 3 States that the media has been arguing are facing a dangerous second wave. The overall mortality is in fact barely higher or even lower than previous years. (source)
Falsity #22: We’re Very Far From Herd Immunity, And Reopening Too Early Is Deadly
“It looks like at least 50% of the population seems to not be susceptible [to COVID] at the present time.” [Note: he also mentioned this proportion could be up to 80%]
— Dr. Karl Friston, considered one of the most influential brain scientist of our time
Many media reports argued that up to 80% of all people needed to have caught COVID and developed antibodies before the pandemic died down on its own — the so-called Herd Immunity everyone has been talking about.
There are now strong indications that the presence of antibodies alone is a poor indicator of how many people have had COVID in the past, and that a T-cell response (you fight off the virus but never actually develop antibodies) might occur in about 80% of cases. If this is proven true, this means that COVID is 5 times more prevalent and 5 times less deadly than previous thought.
This is still subject to scientific debate, but this might explain why:
- On May 31st, leading doctors in Northern Italy were already saying that the virus was essentially gone — even though the prevalence of antibodies in the Italian population was only around 2.5-9%
- In London, there were less than 100 COVID cases detected per day during the entire month of May — even though the antibody prevalence was only around 15%
Some scientists now suggest that the real threshold for COVID Herd Immunity is around 10-20%. This is plausible, and would finally explain why lifting COVID lockdowns has essentially not led to a significant increase of COVID cases, deaths or hospitalizations, virtually anywhere in the world.
- Prof. Sunetra Gupta from Oxford: “I think we will and have already developed Herd Immunity.” (source). Oxford followed up with a study that showed that 10-20% of saturation might be sufficient to reach herd immunity. (source)
- JB Handley – LOCKDOWN LUNACY 2.0: Second wave? Not even close.
- Compiled by Swiss Policy Research:
- “A Swedish study showed that people with mild or asymptomatic disease often neutralized the virus with T-cells without the need to produce antibodies. Overall, T-cell immunity was about twice as common as antibody immunity.
- A large Spanish antibody study published in Lancet showed that less than 20% of symptomatic people and about 2% of asymptomatic people had IgG antibodies.
- A German study (preprint) showed that 81% of the people who had not yet had contact with the new corona virus already had cross-reactive T-cells and thus a certain background immunity (due to contact with previous corona cold viruses).
- A Chinese study in the journal Nature showed that in 40% of asymptomatic persons and in 12.9% of symptomatic persons no IgG antibodies are detectable after the recovery phase.
- Another Chinese study with almost 25,000 clinic employees in Wuhan showed that at most one fifth of the presumably infected employees had IgG antibodies (press article).
- A small French study (preprint) showed that six of eight infected family members of Covid patients developed a temporary T-cell immunity without antibodies.”
- Around the world, several countries like Switzerland, Germany and Canada have started opening up, without any significant increase in COVID-related deaths or hospitalizations.
When Will The Corona Madness End?
“This crisis has been produced entirely, by politicians themselves. There is no REAL existing crisis. So the ‘crisis’ will be over when politicians decide for it to be over. It has nothing to do with the virus.” [emphasis mine]
— Dr. Sucharit Bhakdi, medical doctor and specialist in microbiology, one of the most cited research scientists in German history
This interview from Pathology Professor Dr. John Lee sums up my current thinking perfectly. If there’s one you should watch it’s this one.
Dr. Lee: “Instead of patting ourselves in the back about how well we’ve done with this, how well governments approached this, how well we’ve all pulled together…
We need to be grown up enough to stand back, actually have a look at this and think ‘this was wrong’, ‘it was a mess’, ‘we shouldn’t have done it’ and “how will we be able to deal with this in the future’.” [emphasis mine]
When you step out of the hysteria, it becomes clear that the COVID crisis was a bad flu, at best. In most countries, it’ll barely be seen in statistics of excess mortality.
This crisis has been a crisis of nursing homes, mostly. This is where we still need to focus. Protect those at risk, and stop quarantining the healthy.
Young, healthy people very rarely die from COVID, and the same people who are at risk of dying from the flu or other respiratory illnesses are those affected by this virus. Given the facts presented above, the global reaction to COVID has been completely overblown, hysteric, and as Prof. Bhakdi had predicted back in March, akin to “collective suicide”.
The question is… how long will it take for the Corona-Panic take to subside? When will we finally go back to normal? How much time can politicians try to save face and continue spouting nonsense around how lockdowns saved us all?
I don’t know, to be honest.
When I look at other parts of the world, I see hope: Like when I realized that the city of Prague has set up a 1,600 feet table to celebrate the end of COVID. Everyone sharing food, talking, laughing, singing… no social distancing, no masks, no worries. The “old normal”. Are the Czech the crazy ones, or are we losing it in North America?

Image source: Gabriel Kuchta/Getty Images via CNN Travel (ironically, since no one travels these days)
The truth is slowly coming out in many countries, where politicians are realizing that they probably made a terrible mistake buying into the hysteria:
- Russia: top health official responsible for the COVID response says “it’s all bulls**t. “It’s all exaggerated. It’s an acute respiratory disease with minimal mortality. […] Why has the whole world been destroyed? That I don’t know.”
- United Kingdom: Health officials are starting to admit that COVID was in full retreat before lockdowns were imposed (we already knew this in April…)
- Denmark: Leaked emails show that the Danish Health Authority (who said COVID isn’t that dangerous) didn’t agree with lockdowns and got pushed aside by the government.
- Norway: The prime minister admitted she panicked and locked the country down. Health officials express regrets.
- Germany: A devastating report by the Ministry of the Interior which showed that lockdowns were useless and destructive was ignored by the government, and released anyway by its authors (including scientists from several German universities, stirring massive controversy.
- Switzerland: The Swiss chief physician of infectiology, Pietro Vernazza, admits that lockdowns made little difference, and that the virus was already under control before they were imposed.
Nothing is all black or all white, and I’m doing my best to stay balanced. But one thing is sure: Reality is extremely different from what has been presented so far in the media.
My hope is that by sharing the work of scientists who have been trying to present facts and calm the world down for months, we’ll accelerate the process of getting out of this nonsense.
If you want to stay informed about the latest COVID developments, follow these scientists and public health experts:
- Nobel winner Michael Levitt (Twitter)
- Oxford Center for Evidence-Based Medicine (+ listen to a great interview from Tom Jefferson here)
- Ivor Cummins’ YouTube Channel
- Joel Hay, PhD (Twitter)
- Interviews on UnHerd
- Del Bigtree’s The Highwire (I don’t agree 100% with everything presented, but he has done incredible work on COVID)
- Reporter Alex Berenson (Twitter) — his style is not for everyone but he also has done incredible work
- William M. Briggs’ Blog
- Lockdown Sceptics (UK based)
COVID-ly yours,
Nick
