

Some people claim that 60 percent of all statistics, like this one, is just made up out of thin air. All statistics in relation to Covid – numbers infected, infection and case fatality rates, deaths from and with Covid, the number of lives saved by lockdowns, masks, and vaccines, the number of lives lost in the long term due to lockdown and mask harms and vaccine injuries, the widely-practised disinformation of misclassifying deaths in the first 2-3 weeks following vaccination as ‘unvaccinated’ if the status is unknown or this was the second dose – are open to cherry-picked data being manipulated, with assumptions fed into models to produce pre-determined outputs.
This also makes cross-country comparisons exceptionally challenging, as countries use different definitions of key concepts and different methodologies to estimate the various counts. Still, we must work within these limitations as this is the only data we have.
Data Don’t Back Claims of Vaccine Success
‘Success’ of Covid vaccines in American public perception may arise from the chronological coincidence of the decline in Covid mortality rate that coincided with the vaccine rollout. But by this time sizable numbers of Americans had also been infected by the virus and built up natural immunity that is both more robust and longer-lasting than that conferred by vaccines. In time this eventuates into the public good of herd immunity.
Consider three examples – Australia, New Zealand, and India – that contradict the claim of the beneficial impact of vaccines in driving down the US Covid death rate. The data are drawn from Our World in Data and Worldometers. I will address the safety issues shortly. For now, the key takeaway is, following Karl Popper’s falsifiability test, the three cases demonstrate the ineffectiveness of vaccines.
The US total Covid-related death toll as of 8 April 2024 is 3.6 times as many as died in pre-vaccine 2020. The explanation for this is that only one-third of all US Covid-related deaths were since 1 January 2022, by which date 63.4% of Americans had been fully vaccinated. By contrast, over 90 percent of Australia’s Covid-related deaths occurred since 1 January 2022, when it had reached 75.5% full vaccination. In sharp contrast to the US, therefore, 27.1 times as many Australians died with Covid since 1 January 2022 as in 2020.
New Zealand deaths are even more disproportionately concentrated in the period since 1 January 2022, when 74.4 percent of the population was fully vaccinated. Only 25 people died with Covid in 2020, and by the end of 2021 the total was 50. Yet in April 2024 the total was between 4,000 (Our World in Data) and 5,700 (Worldometers – I have no insight on the discrepancy in numbers between these two data sources). That is, an astonishing 98-99 percent of all Covid-related deaths in the country occurred after hitting 74.4 percent full vaccination.
India’s Covid mortality rate was higher than 1 death per million people for about 7-8 weeks from early May to the end of June 2021, peaking at 2.92 on 29 May 2021. This is the period in which the horrific tales of dumped corpses washing ashore and insufficient capacity of the cremation grounds dominated international news coverage of the dire Indian situation. In this time, India’s full vaccination coverage was just 2-4 percent and the death rate peaked with only three percent of the population having completed the initial Covid-19 vaccination protocol. Thus Covid deaths rose and fell in symmetrical steepness according to some internal logic of the virus that had little relationship to the rollout of vaccines.
Measured by deaths per million people, Worldometers data as of 6 April show Australia with the 108th highest Covid mortality of 228 countries. However, countries that did better than Australia include South Korea, Japan, Vietnam, and India on the Asian mainland, in that order; and Taiwan, Iceland, and Singapore as island countries. Taiwan, of course, should have been a lot more exposed and vulnerable owing to winter conditions, proximity to China, and the volume of cross-strait travel before the alarm was raised in early 2020.
We know by now that the notion of an average Covid infection fatality rate (IFR) is highly misleading as a public health policy tool because of the great variability both by age structure and across the world’s regions. Australia, possibly as an indication of the continuing hold of culture cringe that makes its leaders behave like poor relations of the Anglo-US ‘aristocracy,’ likes to compare itself to Europe and the US. Hence the interminable pats on the back by its officials for their brilliant Covid performance, ignoring the immeasurable advantages of the time bought by the good fortune of being in the Southern Hemisphere in the midst of summer when the disease broke in the Northern Hemisphere, the island geography as a natural barrier to the spread of the virus, the plentiful sunshine and outdoors leisure and recreational activities (though policies rather stupidly did their best to neutralise this natural asset: never underestimate the ability and moths-to-the-flame attraction of politicians for cock-ups), and housing and residential patterns.
Even so, if Australia can compare itself to Europe, then it is equally permissible to locate its performance in Oceania. Here Australia was the fifth worst of 18 countries in Oceania and New Zealand was the second worst (only French Polynesia fared worse).
On 26 March, the Australian Bureau of Statistics (ABS) published its monthly statistics for last year. The baseline average used is for number of deaths in the four years 2017–2019 and 2021. Because 2020 and 2022 were atypically lower and higher, respectively, than average years, they are not included in the ABS methodology for calculating the baseline average.
The first notable thing is the increase in the number of Covid-related deaths from 855 in 2020 to 1,231, 9,840, and 4,387 in the next three years. With assistance from heavy doses of coercion and compulsion for some sectors, the vaccine rollout from early 2021 had achieved extraordinarily high takeup and 95.5 percent of over-16s were double-vaccinated by the end of April 2022. Thus for practical purposes Australia had achieved universal adult vaccination.
And yet, there were 43 percent more deaths in 2021 and a staggering 11.5 times as many deaths in 2022 as in pre-vaccine 2020. In addition, there were more than five times as many deaths in 2023, by which time the pandemic was supposedly over, as in 2020. If this indicates vaccine success, I hate to think what failure would look like.
This contradicts all the bombastic claims of the public health clerisy about the great success of their pandemic management interventions centred on lockdowns, masks, and vaccines. How many times did Prime Minister Scott Morrison claim that his Covid management policies saved 40,000 lives, a made-up statistic that he continues to peddle?
Rather, it vindicates the two core claims of vaccine critics like Stanford University’s Jay Bhattacharya, Oxford’s Sunetra Gupta, and Harvard’s Martin Kulldorff, the three eminent epidemiologists who wrote the Great Barrington Declaration in October 2020. They argued that once a virus is already seeded in the community, it cannot be eradicated but only managed until it becomes endemic and universal. And secondly, the various restrictions on social interactions could delay but would not be able to avoid the final toll. Consequently, the trajectory of the rise and fall of the coronavirus was likely to be policy invariant; that is, not much affected by the different policy interventions. And so it came to pass.
Sweden, Take a Bow
Among countries, the standout proof of this is Sweden, which took the sensible decision of staying with the existing science and policy recommendations based on a hundred years of research, data, and real-world experience, rather than risk the radical evidence-free lockdown and mask measures instituted by panicked governments. Ditto Florida among US states.
Their Covid health outcomes today are no worse than the average for European countries and US states. As per the Worldometers data, the case fatality rate of SARS-CoV-2 is 0.99 percent and the overall survival rate is 98.97 percent. The first may be overstated and the second understated, owing to the less than comprehensive reporting, recording, and data collection of infections among hundreds of millions in developing countries.
Measured by deaths per million people, Sweden was 23rd worst of 47 European countries and 35th worst globally and the US was the 14th worst in the world. Sweden’s economic, educational, and social outcomes are substantially better.
On 11 February, Frederik NG Andersson and Lars Jonung from Lund University in Sweden published a study in Economic Affairs examining the benefits and costs of lockdowns across 25 countries in Europe, with a particular focus on Sweden as the outstanding contrarian on that policy. Their conclusions emphasise the importance of avoiding panic amidst a crisis and not letting short-term decisions undermine long-term outcomes.
Instead, measures introduced without a firm evidence basis as a temporary necessity lasted for two years and authoritarian China served as the model for curtailing civil liberties and citizens’ rights. Europe’s democracies instituted needlessly stringent lockdowns that produced negligible positive health effects but the decline in economic activity did correlate with the severity of lockdowns. This pathology was compounded by efforts to counter the downturn in economic activity with excessively expansionary fiscal and monetary policies that led to ballooning public debt.
By contrast, Sweden’s lockdown restrictions were modest and mostly voluntary and its fiscal response was also restrained. This gave Sweden remarkably low cumulative excess mortality, small losses in economic growth, and continued strong public finances. Sweden’s GDP today is around six percent bigger than in 2019. A 34-country study published in November in the US Proceedings of the National Academy of Sciences concluded that the US ‘would have had 1.60 million fewer deaths if it had the performance of Sweden.’
Let that sink in.
Australia’s Concerning Excess Deaths
The second striking feature of the ABS data is the phenomenon of excess deaths, defined as ‘the difference between the observed number of deaths in a specified time period and the expected numbers of deaths in that same time period.’ Figure 1 is a snapshot of excess deaths in Australia, Sweden, and the US.
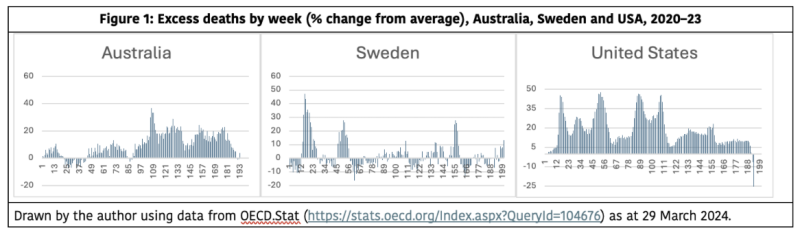
During the Covid years, the ABS explains, excess death estimates were ‘used to provide information about the burden of mortality potentially related to the Covid-19 pandemic, including deaths that are directly or indirectly attributed to Covid-19.’ Notice the sleight of hand (sleight of mind?) here. There is no mention of deaths resulting, either directly or indirectly, from the policies to deal with the pandemic, only from the viral disease itself.
Why does this matter? There is a medical term called ‘iatrogenic,’ defined by the Cambridge Dictionary as a disease or problem ‘caused by medical treatment or by a doctor.’ An example of its use in a sentence is: ‘Over 100,000 deaths occur in North America from iatrogenic disease, which means doctor- or drug-induced disease.’
There has been an extensive debate, out in the real world beyond the one inhabited by the top executives of the major vaccine manufacturers, public health bureaucrats, and the medical establishment, of the full magnitude and severity of Covid-19 vaccine injury, including deaths. Many studies, but not all, have found strong correlations between excess deaths and vaccination rollouts, rates, and number of doses.
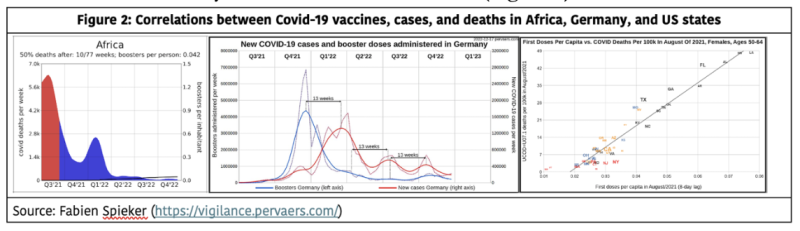
Igor Chudov, for example, found that vaccination rates explain 24 percent of the excess mortality across 31 European countries, which is statistically highly significant. Charts produced by Fabian Spiker include three examples showing the temporal association of spikes in Covid-19 deaths across Africa, the strong correlation between boosters and Covid cases in Germany, and between the first doses of the vaccines and Covid deaths in 50–64-year-old women in US states (Figure 2).
Because billions of Covid vaccines were administered by the revolutionary mRNA platform under emergency use authorisation before the traditional multiyear safety and efficacy tests normally required of new vaccines could be completed, public health authorities and drug regulators should have been extra vigilant about potential iatrogenic harms caused by vaccines. Instead too many seem to have operated as drug enablers rather than regulators.
A major risk-benefit assessment of vaccine boosters for 18-29-year-olds published in the Journal of Medical Ethics in January found that to prevent one Covid hospitalisation of a previously uninfected person, 22,000-30,000 people must be boosted with an mRNA vaccine. But for one hospitalisation prevented, 18-98 serious adverse events can be expected.
The net risk-benefit ratio is in fact even less favourable owing to the high prevalence of post-infection immunity in that population group and the lack of compelling public health benefits, since vaccines have only transient effectiveness against transmission. Mandates cause wider social harms like curtailing access to educational and job opportunities, reputational damage, threats of disenrollment and deportation, generating mistrust in society and public institutions, and fuelling vaccine hesitancy for life-saving paediatric and adult vaccines.
Another study published in February looked at death rates by vaccination status among hospitalised patients with Covid and found that in the over-50s, the vaccinated group had almost double the mortality rate of the unvaccinated group (70-37 percent). Moreover, those with more doses had higher mortality rates.
Professor Carl Heneghan, director of the Centre for Evidence-Based Medicine at Oxford University, and Tom Jefferson ask why the UK Health Security Agency refuses to disclose to Parliament and the public data that it holds on mortality by number of vaccine doses. Could it be because data from the complementary Office of National Statistics show that excess deaths have been primarily in the vaccinated, suggesting but not proving that vaccines may be playing some role?
On 2 March, a cross-party group of 21 British MPs and peers criticised the ‘wall of silence’ on the topic and wrote to Health Secretary Victoria Atkins about the ‘growing public and professional concerns’ at the UK’s rates of excess deaths since 2020. On 21 March, it was announced that the House of Commons will have a debate on excess deaths on 18 April.
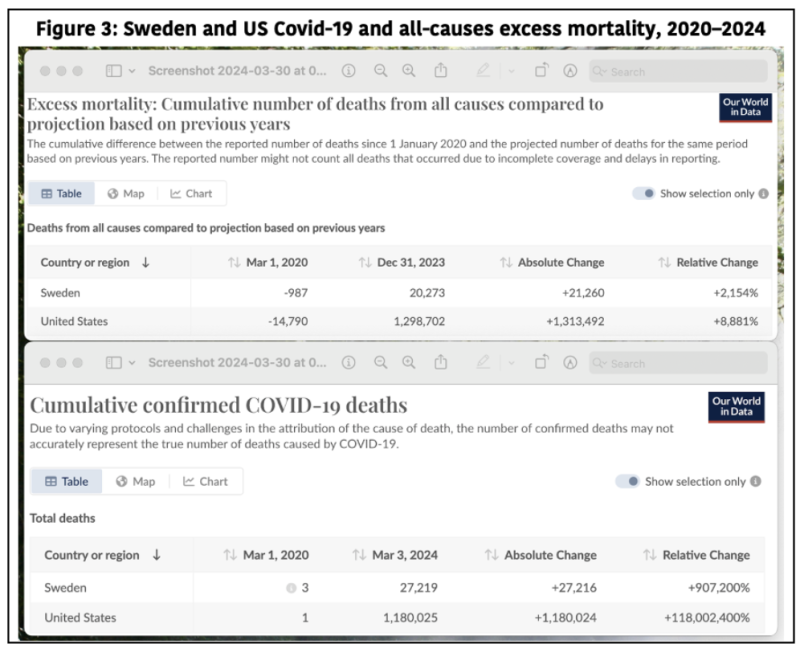
Even with respect to any association between vaccination and excess deaths, however, Sweden is an outlier. It is among the most highly vaccinated countries, achieving 70 percent full vaccination in January 2022 (the US was at 65 and Australia at 77 percent at that time). Sweden’s cumulative excess mortality from 1 March 2020 to 31 December 2023 was 21,260, compared to 51,007 for Australia and 1,313,492 for the US.
But here’s the thing. According to Our World in Data, Sweden’s total Covid-related deaths by 3 March 2024 was 27,219 and that for the US was 1,180,025 (Figure 3).
In other words, Sweden’s non-Covid excess deaths were negative, lower than the baseline average. Because the dates between the two sets of figures are discrepant, I did some creative guesstimating using data from Our World in Data, OECD excess deaths statistics, and the provisional monthly statistics published by the ABS for 2020, 2021, 2022, and 2023. As per these non-authoritative calculations of date-adjusted data, by March this year the net non-Covid excess deaths were 29,367 for Australia, minus 4,574 for Sweden, and 222,016 for the US.
What’s interesting about Sweden, of course, is that this is exactly the result we would expect with Covid having killed substantial numbers of the vulnerable population of the elderly and the comorbid, thereby reducing the cohort at serious risk of death in the subsequent few years. Be that as it may, Sweden’s example once again suggests that the enduring harms of lockdown restrictions might possibly have significant explanatory potency for the stubbornly persistent excess deaths. Or did Sweden just strike it lucky with its particular batches of the vaccines, as there seems to be some evidence that not all batches were equal in the quality control during the manufacturing process?
Returning to Australia, the non-Covid number of excess deaths was 16,046 in 2022 (9.7 percent) and 12,345 last year (7.5 percent). There’s no conclusive evidence that vaccination is a or the primary cause of excess mortality. But there are enough concerning safety signals that the matter needs proper investigation in conjunction with the persistent patterns of harms from the lockdown social experiment. Refusing to investigate this is especially odd after the insistence since 2020 that even one avoidable Covid death is one death too many. Hence the insistence on shutting down an entire city or state with the detection of just one Covid case.
After repeated failed attempts, on 26 March the Senate voted 31-30 to hold an inquiry by the Community Affairs References Committee into factors contributing to excess deaths. Senator Ralph Babet, the prime instigator behind the motion, thinks this might be a world-first inquiry.
Remarkably, all the Green and Labor senators voted against this. Seriously? What do they fear will be revealed that they would rather keep hidden?
In striking contrast to the enthusiastic vaccine takeup in 2021–22, in the six months to March this year, only 3.3 percent of 18-64-year-olds had received a booster and in the much more vulnerable 65-74-year-olds, 21.4 percent, according to the Department of Health.
Clearly, most people are done with Covid and have stopped paying heed to the advice from public health authorities. This of course contains its own long-term dangers. Are Labor and the Greens not interested in knowing the vaccine truth and restoring public trust in the integrity of our public institutions, including Health and Parliament?
A substantially shorter version of this was published in the Spectator Australia on 13 April.
Disclaimer
Some of the posts we share are controversial and we do not necessarily agree with them in the whole extend. Sometimes we agree with the content or part of it but we do not agree with the narration or language. Nevertheless we find them somehow interesting, valuable and/or informative or we share them, because we strongly believe in freedom of speech, free press and journalism. We strongly encourage you to have a critical approach to all the content, do your own research and analysis to build your own opinion.
We would be glad to have your feedback.

Source: Brownstone Institute Read the original article here: https://brownstone.org/